

2013 ACC/AHA Cholesterol Guideline Versus 2004 NCEP ATP III Guideline in the Prediction of Coronary Artery Calcification Progression in a Korean Population
- PMID: 27543305
- PMCID: PMC5015275
- DOI: 10.1161/JAHA.116.003410
2013 ACC/AHA Cholesterol Guideline Versus 2004 NCEP ATP III Guideline in the Prediction of Coronary Artery Calcification Progression in a Korean Population
Abstract
Background: Since the release of the 2013 American College of Cardiology/American Heart Association (ACC/AHA) guidelines, significant controversy has surrounded the applicability of the new cholesterol guidelines and the Pooled Cohort Equations. In this present study, we investigated whether eligibility for statin therapy determined by the 2013 ACC/AHA guidelines on the management of blood cholesterol is better aligned with the progression of coronary artery calcification (CAC) detected by coronary computed tomography angiography (CCTA) than the previously recommended 2004 National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III guidelines.
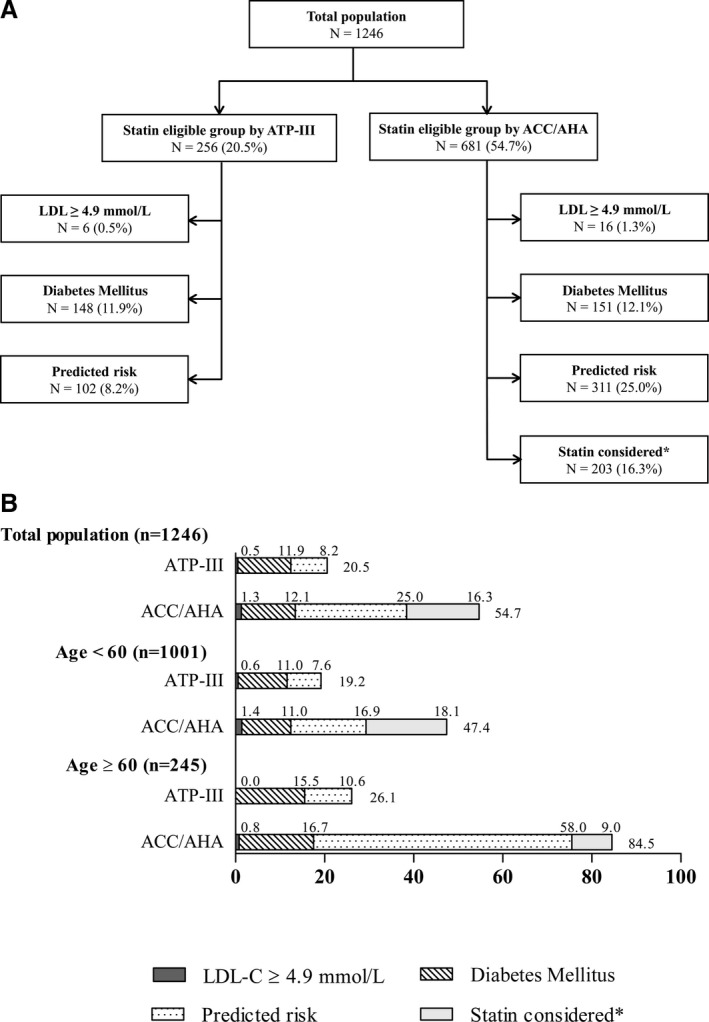
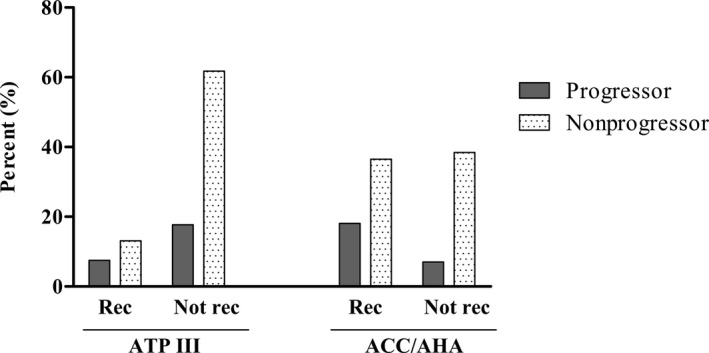
Methods and results: We enrolled 1246 asymptomatic participants who underwent repeated CAC score measurement during routine health examinations. The CAC score progression was defined as either incident CAC in a population free of CAC at baseline or increase ≥2.5 units between the baseline and final square root of CAC scores participants who had detectable CAC at baseline examination. Application of the ACC/AHA guidelines to the study population increased the proportion of statin-eligible subjects from 20.5% (according to ATP III) to 54.7%. Statin-eligible subjects, as defined by ACC/AHA guidelines, showed a higher odds ratio for CAC score progression than those considered statin eligible according to ATP III guidelines (2.73 [95% CI, 2.07-3.61] vs 2.00 [95% CI, 1.49-2.68]).
Conclusions: Compared with the ATP III guidelines, the new ACC/AHA guidelines result in better discrimination of subjects with cardiovascular risk detected by CAC score progression in an Asian population.
Keywords: Pooled Cohort Equation; atherosclerosis; cardiovascular disease; cholesterol guidelines; coronary artery calcification.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
Comment in
-
Preventing Atherosclerotic Cardiovascular Disease Using American College of Cardiology and American Heart Association Prevention Guidelines: Some Good News, But Caveats Remain.J Am Heart Assoc. 2016 Aug 19;5(8):e004197. doi: 10.1161/JAHA.116.004197. J Am Heart Assoc. 2016. PMID: 27543310 Free PMC article. No abstract available.
References
-
- Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, Goldberg AC, Gordon D, Levy D, Lloyd‐Jones DM, McBride P, Schwartz JS, Shero ST, Smith SC Jr, Watson K, Wilson PW, Eddleman KM, Jarrett NM, LaBresh K, Nevo L, Wnek J, Anderson JL, Halperin JL, Albert NM, Bozkurt B, Brindis RG, Curtis LH, DeMets D, Hochman JS, Kovacs RJ, Ohman EM, Pressler SJ, Sellke FW, Shen WK, Smith SC Jr, Tomaselli GF. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American college of cardiology/American heart association task force on practice guidelines. Circulation. 2014;129:S1–45. - PubMed
-
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults . Executive summary of the third report of the national cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III). JAMA. 2001;285:2486–2497. - PubMed
-
- Kavousi M, Leening MJ, Nanchen D, Greenland P, Graham IM, Steyerberg EW, Ikram MA, Stricker BH, Hofman A, Franco OH. Comparison of application of the ACC/AHA guidelines, adult treatment panel III guidelines, and European society of cardiology guidelines for cardiovascular disease prevention in a European cohort. JAMA. 2014;311:1416–1423. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
