

Childhood amblyopia: current management and new trends
- PMID: 27543498
- PMCID: PMC5862311
- DOI: 10.1093/bmb/ldw030
Childhood amblyopia: current management and new trends
Abstract
Introduction or background: With a prevalence of 2-5%, amblyopia is the most common vision deficit in children in the UK and the second most common cause of functional low vision in children in low-income countries.
Sources of data: Pubmed, Cochrane library and clinical trial registries (clinicaltrials.gov, ISRCTN, UKCRN portfolio database).
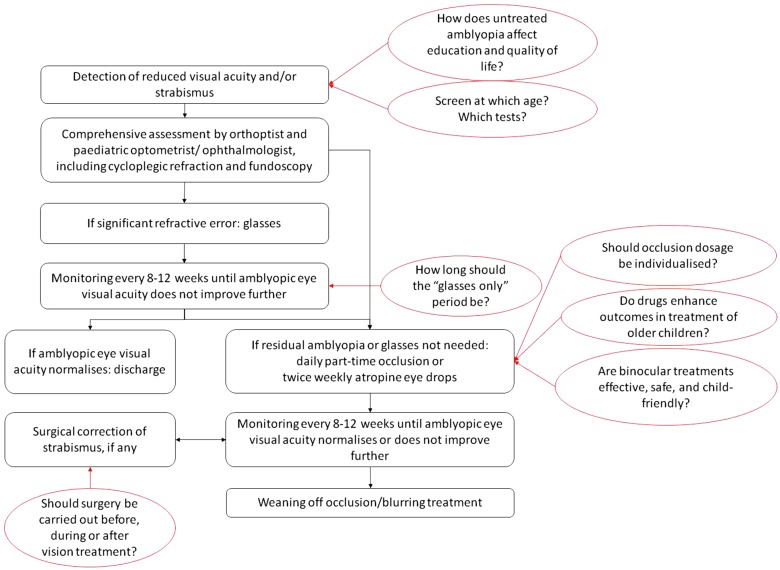
Areas of agreement: Screening and treatment at the age of 4-5 years are cost efficient and clinically effective. Optical treatment (glasses) alone can improve visual acuity, with residual amblyopia treated by part-time occlusion or pharmacological blurring of the better-seeing eye. Treatment after the end of the conventional 'critical period' can improve vision, but in strabismic amblyopia carries a low risk of double vision.
Areas of controversy: It is not clear whether earlier vision screening would be cost efficient and associated with better outcomes. Optimization of treatment by individualized patching regimes or early start of occlusion, and novel binocular treatment approaches may enhance adherence to treatment, provide better outcomes and shorten treatment duration.
Growing points: Binocular treatments for amblyopia.
Areas timely for developing research: Impact of amblyopia on education and quality of life; optimal screening timing and tests; optimal administration of conventional treatments; development of child-friendly, effective and safe binocular treatments.
Keywords: amblyopia*/diagnosis; amblyopia*/therapy; child; humans; treatment outcome; vision screening; visual acuity.
© The Author 2016. Published by Oxford University Press. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures

References
-
- Carlton J, Karnon J, Czoski-Murray C, et al. . The clinical effectiveness and cost-effectiveness of screening programmes for amblyopia and strabismus in children up to the age of 4-5 years: a systematic review and economic evaluation. Health Technol Assess 2008;12:iii, xi–194. - PubMed
-
- Powell C, Hatt SR. Vision screening for amblyopia in childhood. Cochrane Database Syst Rev 2009;3:CD005020. - PubMed
-
- Gilbert CE, Ellwein LB. Prevalence and causes of functional low vision in school-age children: results from standardized population surveys in Asia, Africa, and Latin America. Invest Ophthalmol Vis Sci 2008;49:877–81. - PubMed
-
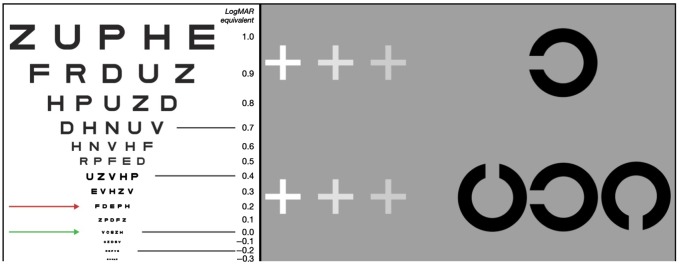
- Norgett Y, Siderov J. Crowding in children's visual acuity tests--effect of test design and age. Optom Vis Sci 2011;88:920–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
