

Use of Intravascular Imaging During Chronic Total Occlusion Percutaneous Coronary Intervention: Insights From a Contemporary Multicenter Registry
- PMID: 27543800
- PMCID: PMC5015304
- DOI: 10.1161/JAHA.116.003890
Use of Intravascular Imaging During Chronic Total Occlusion Percutaneous Coronary Intervention: Insights From a Contemporary Multicenter Registry
Abstract
Background: Intravascular imaging can facilitate chronic total occlusion (CTO) percutaneous coronary intervention.
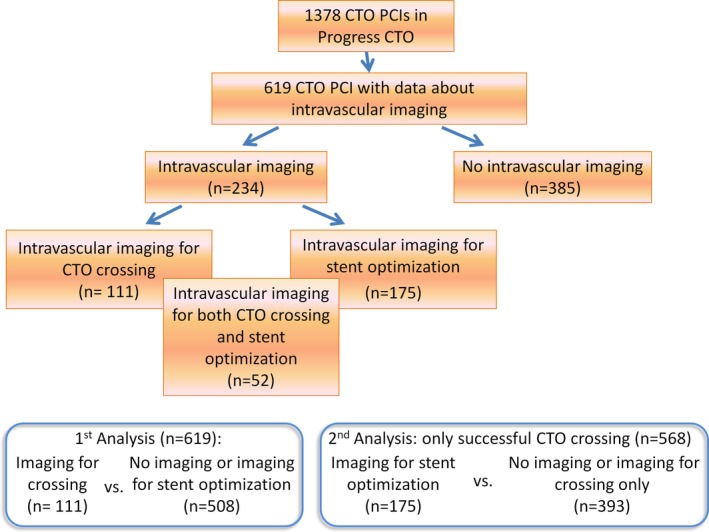
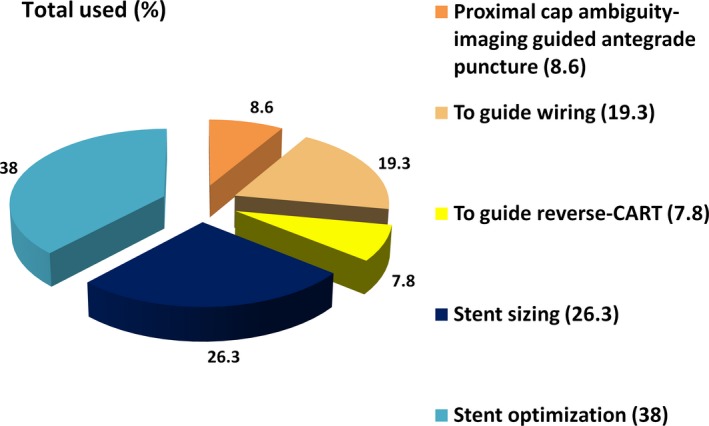
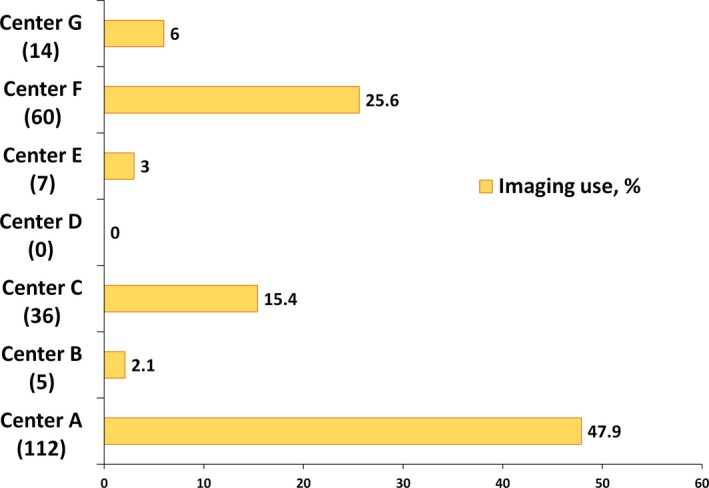
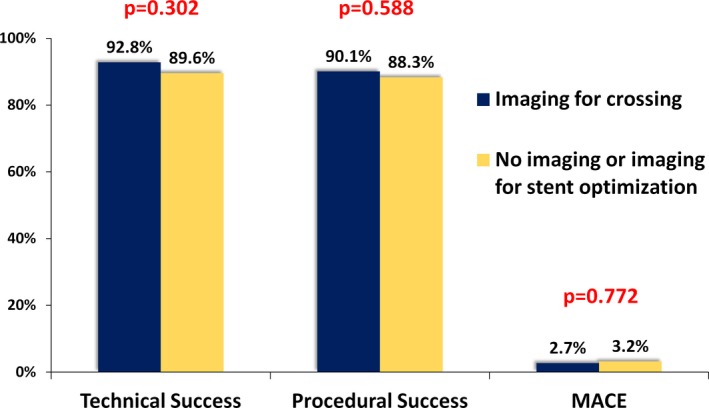
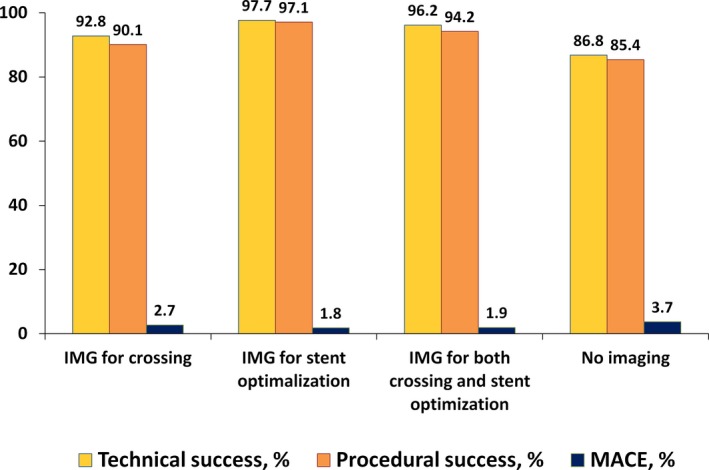
Methods and results: We examined the frequency of use and outcomes of intravascular imaging among 619 CTO percutaneous coronary interventions performed between 2012 and 2015 at 7 US centers. Mean age was 65.4±10 years and 85% of the patients were men. Intravascular imaging was used in 38%: intravascular ultrasound in 36%, optical coherence tomography in 3%, and both in 1.45%. Intravascular imaging was used for stent sizing (26.3%), stent optimization (38.0%), and CTO crossing (35.7%, antegrade in 27.9%, and retrograde in 7.8%). Intravascular imaging to facilitate crossing was used more frequently in lesions with proximal cap ambiguity (49% versus 26%, P<0.0001) and with retrograde as compared with antegrade-only cases (67% versus 31%, P<0.0001). Despite higher complexity (Japanese CTO score: 2.86±1.19 versus 2.43±1.19, P=0.001), cases in which imaging was used for crossing had similar technical and procedural success (92.8% versus 89.6%, P=0.302 and 90.1% versus 88.3%, P=0.588, respectively) and similar incidence of major cardiac adverse events (2.7% versus 3.2%, P=0.772). Use of intravascular imaging was associated with longer procedure (192 minutes [interquartile range 130, 255] versus 131 minutes [90, 192], P<0.0001) and fluoroscopy (71 minutes [44, 93] versus 39 minutes [25, 69], P<0.0001) time.
Conclusions: Intravascular imaging is frequently performed during CTO percutaneous coronary intervention both for crossing and for stent selection/optimization. Despite its use in more complex lesion subsets, intravascular imaging was associated with similar rates of technical and procedural success for CTO percutaneous coronary intervention.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT02061436.
Keywords: chronic total occlusion; intravascular ultrasound; optical coherence tomography; percutaneous coronary intervention.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Hong SJ, Kim BK, Shin DH, Kim JS, Hong MK, Gwon HC, Kim HS, Yu CW, Park HS, Chae IH, Rha SW, Lee SH, Kim MH, Hur SH, Jang Y. Usefulness of intravascular ultrasound guidance in percutaneous coronary intervention with second‐generation drug‐eluting stents for chronic total occlusions (from the Multicenter Korean‐Chronic Total Occlusion Registry). Am J Cardiol. 2014;114:534–540. - PubMed
-
- Tian NL, Gami SK, Ye F, Zhang JJ, Liu ZZ, Lin S, Ge Z, Shan SJ, You W, Chen L, Zhang YJ, Mintz G, Chen SL. Angiographic and clinical comparisons of intravascular ultrasound‐ versus angiography‐guided drug‐eluting stent implantation for patients with chronic total occlusion lesions: two‐year results from a randomised AIR‐CTO study. EuroIntervention. 2015;10:1409–1417. - PubMed
-
- Kim BK, Shin DH, Hong MK, Park HS, Rha SW, Mintz GS, Kim JS, Lee SJ, Kim HY, Hong BK, Kang WC, Choi JH, Jang Y. Clinical impact of intravascular ultrasound‐guided chronic total occlusion intervention with zotarolimus‐eluting versus biolimus‐eluting stent implantation: randomized study. Circ Cardiovasc Interv. 2015;8:e002592. - PubMed
-
- Park Y, Park HS, Jang GL, Lee DY, Lee H, Lee JH, Kang HJ, Yang DH, Cho Y, Chae SC, Jun JE, Park WH. Intravascular ultrasound guided recanalization of stumpless chronic total occlusion. Int J Cardiol. 2011;148:174–178. - PubMed
-
- Matsubara T, Murata A, Kanyama H, Ogino A. Ivus‐guided wiring technique: promising approach for the chronic total occlusion. Catheter Cardiovasc Interv. 2004;61:381–386. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
