

Targeted Near-Infrared Fluorescence Imaging of Atherosclerosis: Clinical and Intracoronary Evaluation of Indocyanine Green
- PMID: 27544892
- PMCID: PMC5136528
- DOI: 10.1016/j.jcmg.2016.01.034
Targeted Near-Infrared Fluorescence Imaging of Atherosclerosis: Clinical and Intracoronary Evaluation of Indocyanine Green
Abstract
Objectives: This study sought to determine whether indocyanine green (ICG)-enhanced near-infrared fluorescence (NIRF) imaging can illuminate high-risk histologic plaque features of human carotid atherosclerosis, and in coronary atheroma of living swine, using intravascular NIRF-optical coherence tomography (OCT) imaging.
Background: New translatable imaging approaches are needed to identify high-risk biological signatures of atheroma. ICG is a U.S. Food and Drug Administration-approved NIRF imaging agent that experimentally targets plaque macrophages and lipid in areas of enhanced endothelial permeability. However, it is unknown whether ICG can target atheroma in patients.
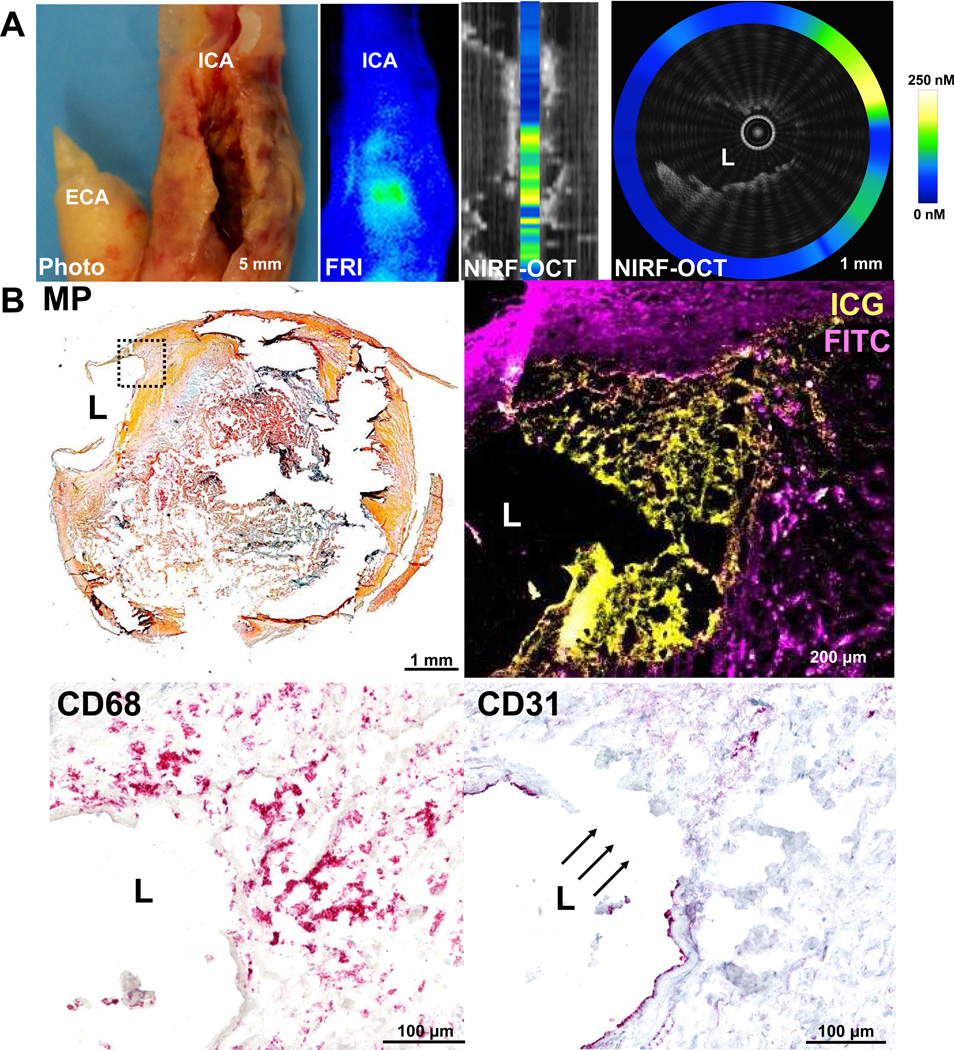
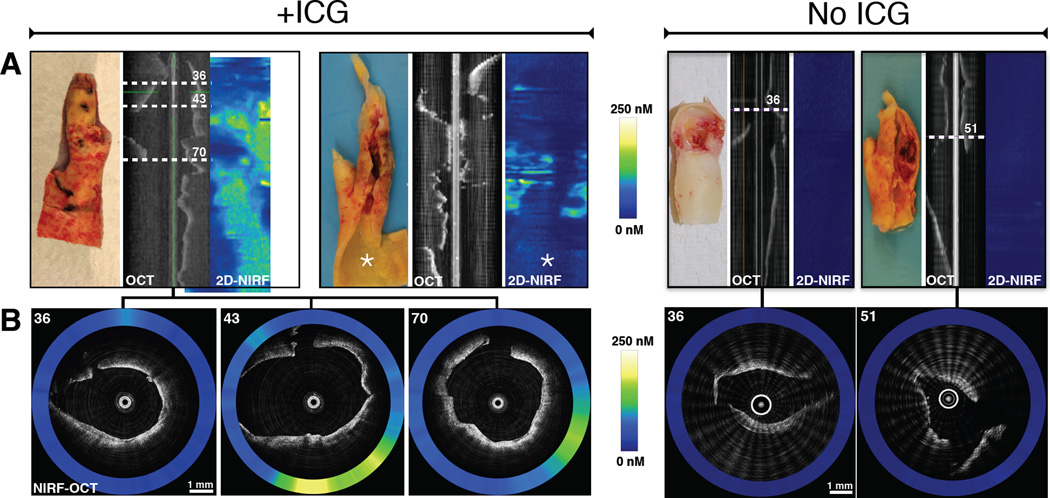
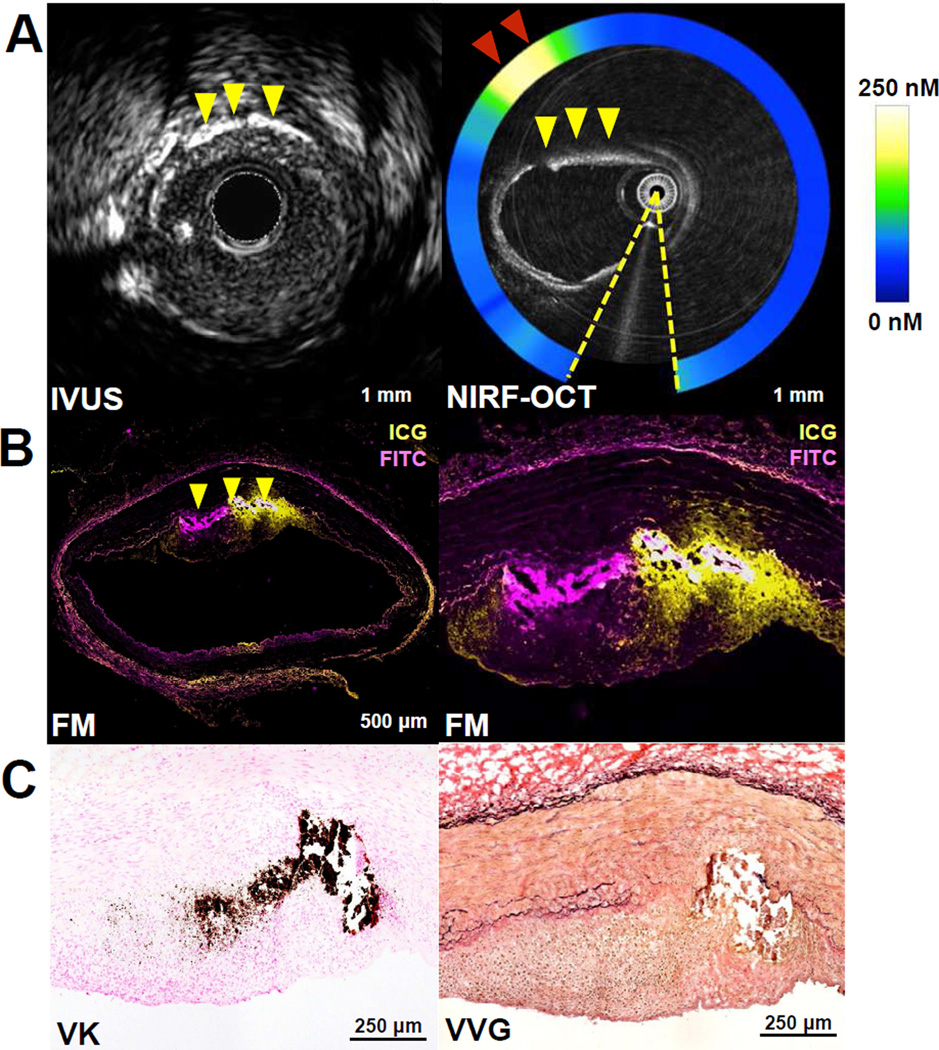
Methods: Eight patients were enrolled in the BRIGHT-CEA (Indocyanine Green Fluorescence Uptake in Human Carotid Artery Plaque) trial. Five patients were injected intravenously with ICG 99 ± 25 min before clinically indicated carotid endarterectomy. Three saline-injected endarterectomy patients served as control subjects. Excised plaques underwent analysis by intravascular NIRF-OCT, reflectance imaging, microscopy, and histopathology. Next, following ICG intravenous injection, in vivo intracoronary NIRF-OCT and intravascular ultrasound imaged 3 atheroma-bearing coronary arteries of a diabetic, cholesterol-fed swine.
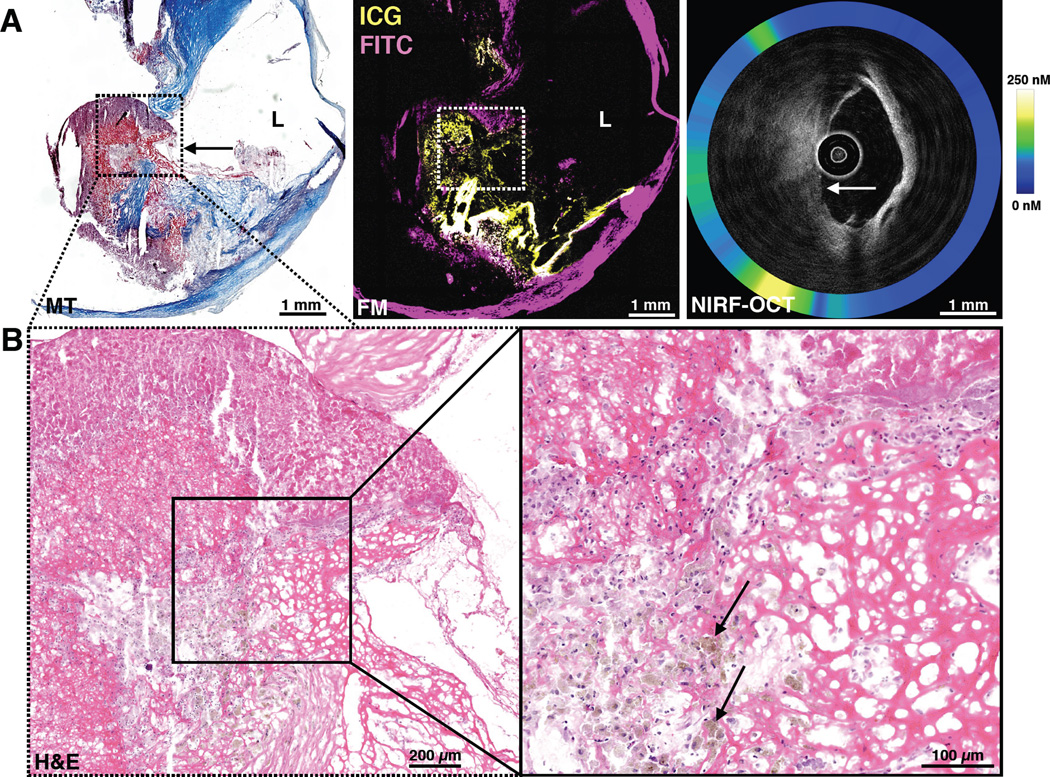
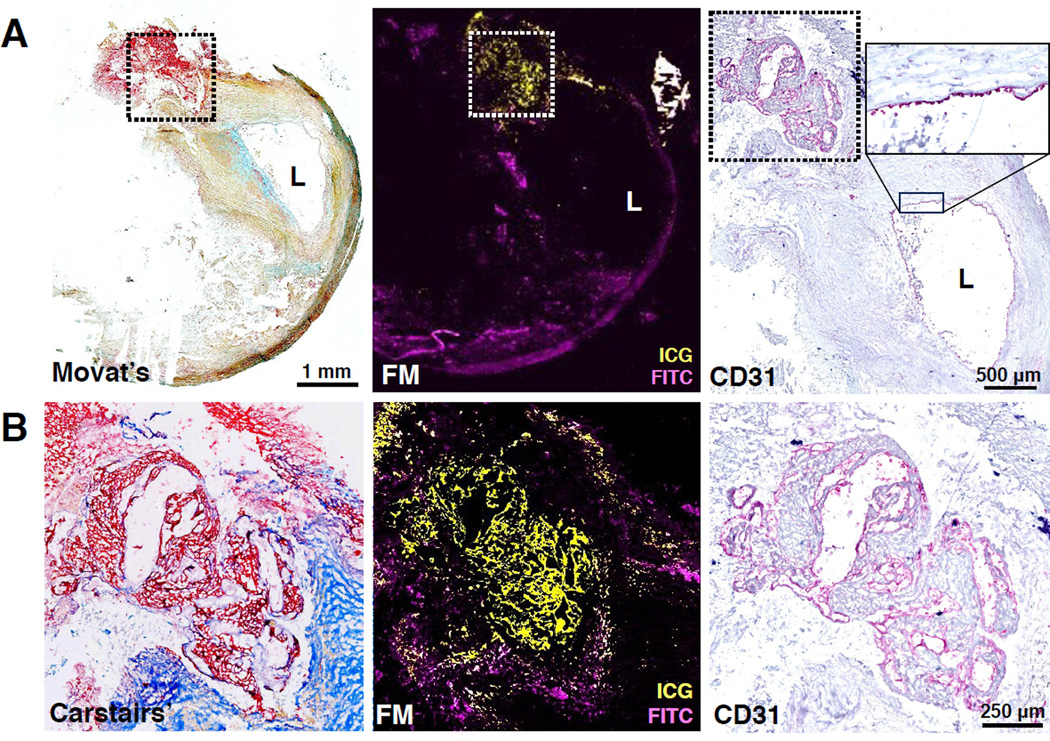
Results: ICG was well tolerated; no adverse clinical events occurred up to 30 days post-injection. Multimodal NIRF imaging including intravascular NIRF-OCT revealed that ICG accumulated in all endarterectomy specimens. Plaques from saline-injected control patients exhibited minimal NIRF signal. In the swine experiment, intracoronary NIRF-OCT identified ICG uptake in all intravascular ultrasound-identified plaques in vivo. On detailed microscopic evaluation, ICG localized to plaque areas exhibiting impaired endothelial integrity, including disrupted fibrous caps, and within areas of neovascularization. Within human plaque areas of endothelial abnormality, ICG was spatially related to localized zones of plaque macrophages and lipid, and, notably, intraplaque hemorrhage.
Conclusions: This study demonstrates that ICG targets human plaques exhibiting endothelial abnormalities and provides new insights into its targeting mechanisms in clinical and experimental atheroma. Intracoronary NIRF-OCT of ICG may offer a novel, clinically translatable approach to image pathobiological aspects of coronary atherosclerosis. (Indocyanine Green Fluorescence Uptake in Human Carotid Artery Plaque [BRIGHT-CEA]; NCT01873716).
Keywords: atherosclerosis; endothelium; indocyanine green; inflammation; intraplaque hemorrhage; intravascular imaging; lipid; molecular imaging; near-infrared fluorescence.
Copyright © 2016 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Going Green for Vulnerable Plaque Detection?JACC Cardiovasc Imaging. 2016 Sep;9(9):1096-1098. doi: 10.1016/j.jcmg.2016.02.032. Epub 2016 Aug 17. JACC Cardiovasc Imaging. 2016. PMID: 27544891 No abstract available.
References
-
- Hope-Ross M, Yannuzzi LA, Gragoudas ES, et al. Adverse reactions due to indocyanine green. Ophthalmology. 1994;101:529–533. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
