

Characteristics of Missed Simultaneous Gastric Lesions Based on Double-Check Analysis of the Endoscopic Image
- PMID: 27545277
- PMCID: PMC5475516
- DOI: 10.5946/ce.2016.056
Characteristics of Missed Simultaneous Gastric Lesions Based on Double-Check Analysis of the Endoscopic Image
Abstract
Background/aims: The detection of multifocal lesions is important for the successful management of gastric neoplasms. We investigated the characteristics of missed simultaneous lesions and the reason for the missed diagnoses.
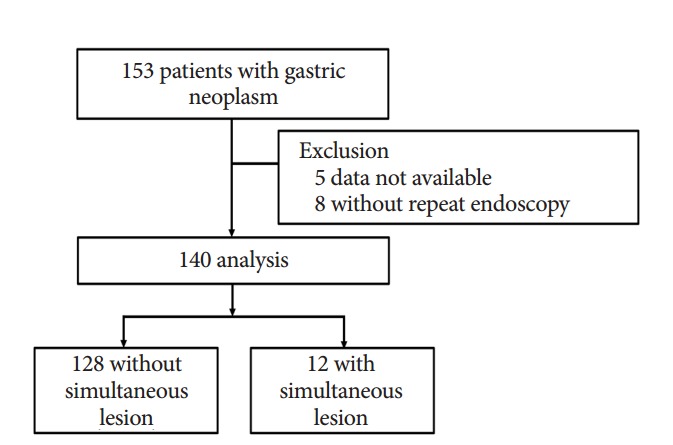
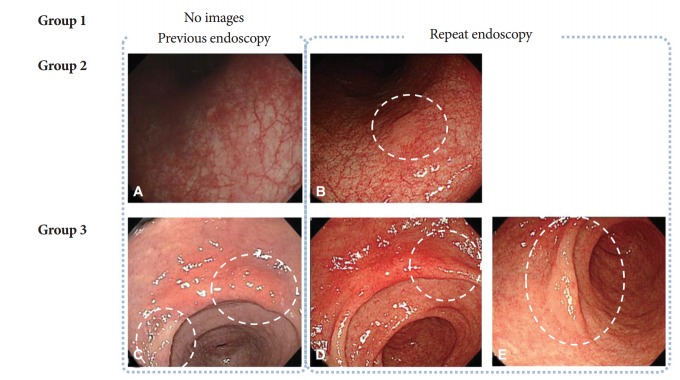
Methods: A total of 140 patients who underwent repeat endoscopy before endoscopic resection between June 2013 and June 2014 were retrospectively reviewed. We classified simultaneous lesions into three groups based on a review of earlier images: group 1, no images of the location of simultaneous lesions were taken; group 2, no corresponding lesion was evident in the previous images; and group 3, simultaneous lesions were visible in the earlier images but a biopsy was not performed.
Results: Simultaneous lesions were found in 12 patients (8.6%) with 13 lesions, comprising 10 dysplasia (76.9%) and three adenocarcinoma (23.1%). Regarding the reasons for missed diagnoses, seven lesions (53.8%) were classified as group 3, five (38.5%) as group 1, and the remaining lesion (7.7%) as group 2. There were no significant differences in the characteristics of the patients with and without simultaneous lesions.
Conclusions: Lesions disregarded or unnoticed during endoscopic examination were the main reason for missed diagnosis of simultaneous lesions. Endoscopists should consider the possibility of simultaneous lesions and attempt to meticulously evaluate the entire gastric mucosa.
Keywords: Endoscopy; Quality; Stomach neoplasms.
Conflict of interest statement
Figures
References
-
- Ahn JY, Jung HY, Choi KD, et al. Endoscopic and oncologic outcomes after endoscopic resection for early gastric cancer: 1370 cases of absolute and extended indications. Gastrointest Endosc. 2011;74:485–493. - PubMed
-
- Choi MK, Kim GH, Park DY, et al. Long-term outcomes of endoscopic submucosal dissection for early gastric cancer: a single-center experience. Surg Endosc. 2013;27:4250–4258. - PubMed
-
- Gong EJ, Ahn JY, Jung HY, et al. Risk factors and clinical outcomes of gastric cancer identified by screening endoscopy: a case-control study. J Gastroenterol Hepatol. 2014;29:301–309. - PubMed
-
- Voutilainen ME, Juhola MT. Evaluation of the diagnostic accuracy of gastroscopy to detect gastric tumours: clinicopathological features and prognosis of patients with gastric cancer missed on endoscopy. Eur J Gastroenterol Hepatol. 2005;17:1345–1349. - PubMed
-
- Lee HL, Eun CS, Lee OY, et al. When do we miss synchronous gastric neoplasms with endoscopy? Gastrointest Endosc. 2010;71:1159–1165. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
