

Sleep disturbance in patients taking opioid medication for chronic back pain
- PMID: 27545291
- PMCID: PMC5082544
- DOI: 10.1111/anae.13601
Sleep disturbance in patients taking opioid medication for chronic back pain
Abstract
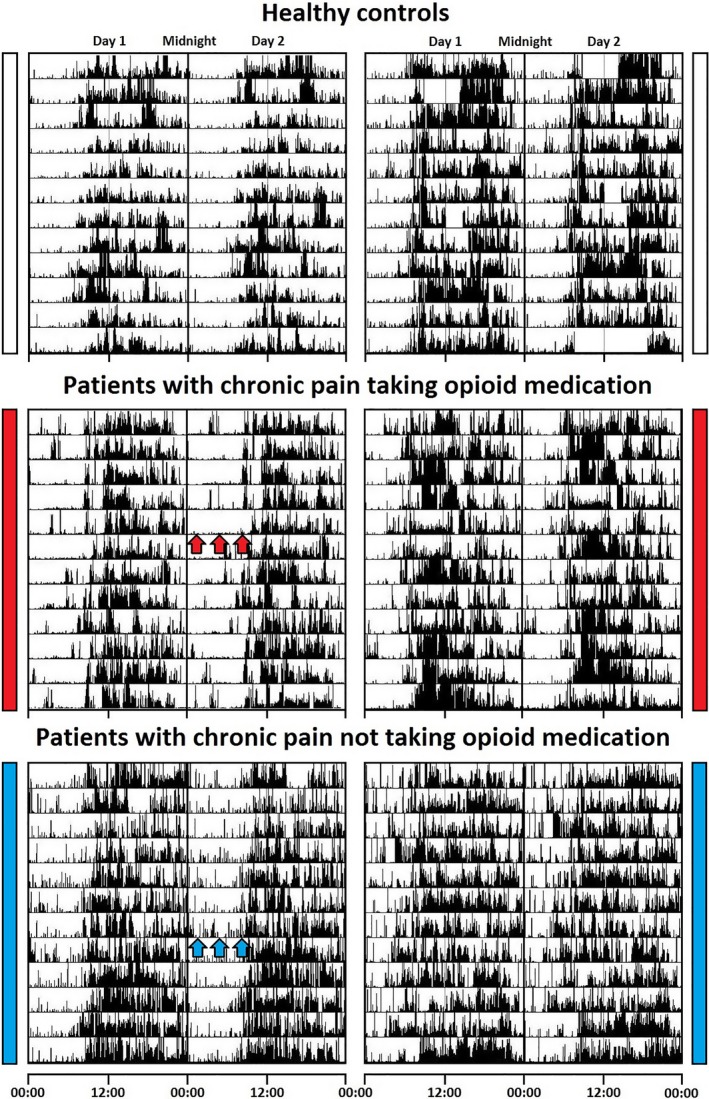
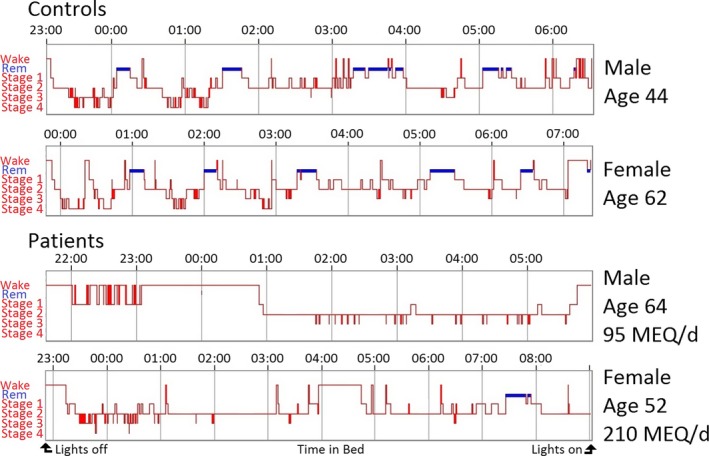
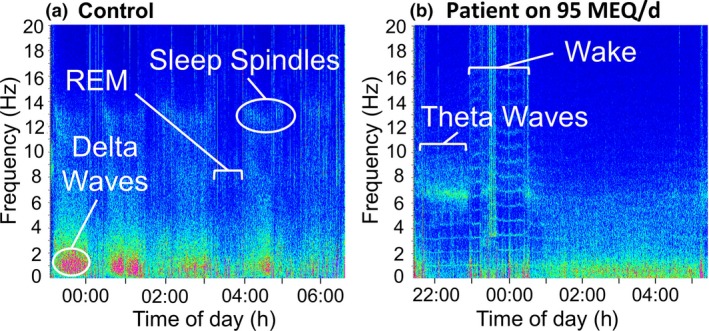
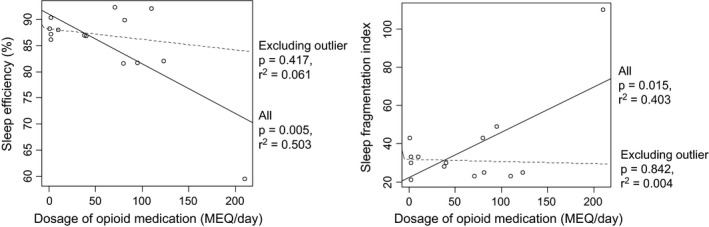
Poor sleep is an increasingly recognised problem with chronic pain and further increases the effect on daily function. To identify the relationship between chronic pain, opioid analgesia and sleep quality, this study investigated activity and sleep patterns in patients taking opioid and non-opioid analgesia for chronic back pain. Thirty-one participants (10 healthy controls, 21 patients with chronic pain: 6 on non-opioid medication; 15 on opioid medication) were assessed using actigraphy, polysomnography and questionnaires. Patients with chronic pain subjectively reported significant sleep and wake disturbances as shown by decreased overall sleep quality (Pittsburgh Sleep Quality Index, p < 0.001), increased symptoms of insomnia (Insomnia Severity Index, p < 0.001) and increased fatigue (Fatigue Severity Scale, p = 0.002). They also spent increased time in bed (p = 0.016), took longer to get to sleep (p = 0.005) and had high interindividual variability in other measures of activity but no overall irregular rest-activity pattern. Patients on high doses of opioids (> 100 mg morphine-equivalent/day) demonstrated distinctly abnormal brain activity during sleep suggesting that polysomnography is necessary to detect sleep disturbance in this population in the absence of irregular rest-activity behaviour. Night-time sleep disturbance is common in individuals suffering from chronic pain and may be further exacerbated by opioid treatment. Considerations must be made regarding the appropriate use of combined actigraphy and miniaturised polysomnography for future population-based studies.
Keywords: chronic opioids: side effects; chronic pain; sleep disturbance.
© 2016 The Authors. Anaesthesia published by John Wiley & Sons Ltd on behalf of Association of Anaesthetists of Great Britain and Ireland.
Figures
Similar articles
-
Towards a better understanding of increased sleep duration in the chronic phase of moderate to severe traumatic brain injury: an actigraphy study.Sleep Med. 2019 Jul;59:67-75. doi: 10.1016/j.sleep.2018.11.012. Epub 2018 Nov 28. Sleep Med. 2019. PMID: 30578112
-
Relationship of chronic pain and opioid use with respiratory disturbance during sleep.Pain Manag Nurs. 2012 Jun;13(2):70-9. doi: 10.1016/j.pmn.2010.04.003. Epub 2010 Nov 19. Pain Manag Nurs. 2012. PMID: 22652280
-
Objective and subjective assessment of sleep in chronic low back pain patients compared with healthy age and gender matched controls: a pilot study.BMC Musculoskelet Disord. 2009 Oct 2;10:122. doi: 10.1186/1471-2474-10-122. BMC Musculoskelet Disord. 2009. PMID: 19799778 Free PMC article.
-
Assessing and Managing Sleep Disturbance in Patients with Chronic Pain.Anesthesiol Clin. 2016 Jun;34(2):379-93. doi: 10.1016/j.anclin.2016.01.007. Anesthesiol Clin. 2016. PMID: 27208716 Review.
-
Opioids and the management of chronic severe pain in the elderly: consensus statement of an International Expert Panel with focus on the six clinically most often used World Health Organization Step III opioids (buprenorphine, fentanyl, hydromorphone, methadone, morphine, oxycodone).Pain Pract. 2008 Jul-Aug;8(4):287-313. doi: 10.1111/j.1533-2500.2008.00204.x. Epub 2008 May 23. Pain Pract. 2008. PMID: 18503626
Cited by
-
The Moderating Role of Fatigue Sensitivity in the Relation between Depression and Alcohol and Opioid Misuse among Adults with Chronic Low Back Pain.Fatigue. 2020;8(3):130-143. doi: 10.1080/21641846.2020.1818933. Epub 2020 Sep 10. Fatigue. 2020. PMID: 34350064 Free PMC article.
-
Opioid suppression of conditioned anticipatory brain responses to breathlessness.Neuroimage. 2017 Apr 15;150:383-394. doi: 10.1016/j.neuroimage.2017.01.005. Epub 2017 Jan 3. Neuroimage. 2017. PMID: 28062251 Free PMC article. Clinical Trial.
-
Pain intensity as a moderator of the association between opioid use and insomnia symptoms among adults with chronic pain.Sleep Med. 2018 Dec;52:98-102. doi: 10.1016/j.sleep.2018.08.015. Epub 2018 Sep 5. Sleep Med. 2018. PMID: 30296735 Free PMC article.
-
Pain Management in the Most Vulnerable Intellectual Disability: A Review.Pain Ther. 2023 Aug;12(4):939-961. doi: 10.1007/s40122-023-00526-w. Epub 2023 Jun 7. Pain Ther. 2023. PMID: 37284926 Free PMC article. Review.
-
Mu-opioid receptor-expressing neurons in the paraventricular thalamus modulate chronic morphine-induced wake alterations.Transl Psychiatry. 2023 Mar 3;13(1):78. doi: 10.1038/s41398-023-02382-w. Transl Psychiatry. 2023. PMID: 36869037 Free PMC article.
References
-
- Palermo TM, Kiska R. Subjective sleep disturbances in adolescents with chronic pain: relationship to daily functioning and quality of life. Journal of Pain 2005; 6: 201–7. - PubMed
-
- McCracken LM, Iverson GL. Disrupted sleep patterns and daily functioning in patients with chronic pain. Pain Research and Management 2002; 7: 75–9. - PubMed
-
- Wulff K, Gatti S, Wettstein JG, Foster RG. Sleep and circadian rhythm disruption in psychiatric and neurodegenerative disease. Nature Reviews Neuroscience 2010; 11: 589–99. - PubMed
-
- Wittig R, Zorick FJ, Blumer D, Heilbronn M, Roth T. Disturbed sleep in patients complaining of chronic pain. Journal of Nervous and Mental Disease 1982; 170: 429–31. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
