

Clinical practice guideline for the prevention, early detection, diagnosis, management and follow up of type 2 diabetes mellitus in adults
- PMID: 27546934
- PMCID: PMC4975132
Clinical practice guideline for the prevention, early detection, diagnosis, management and follow up of type 2 diabetes mellitus in adults
Abstract
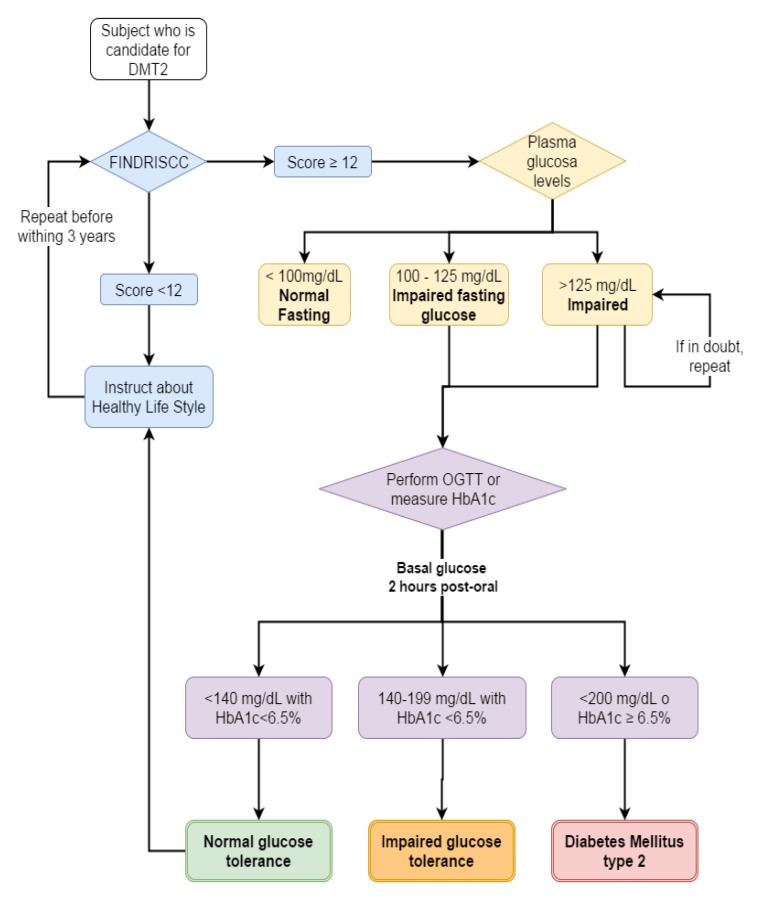
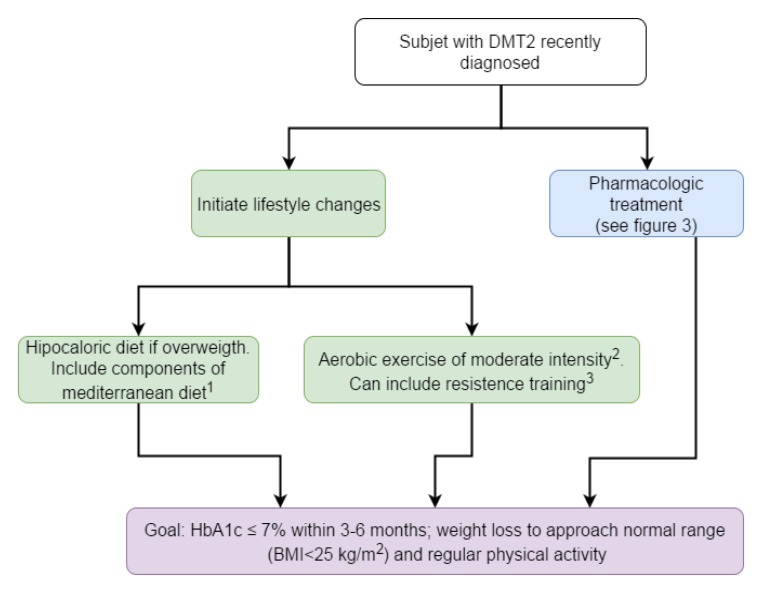
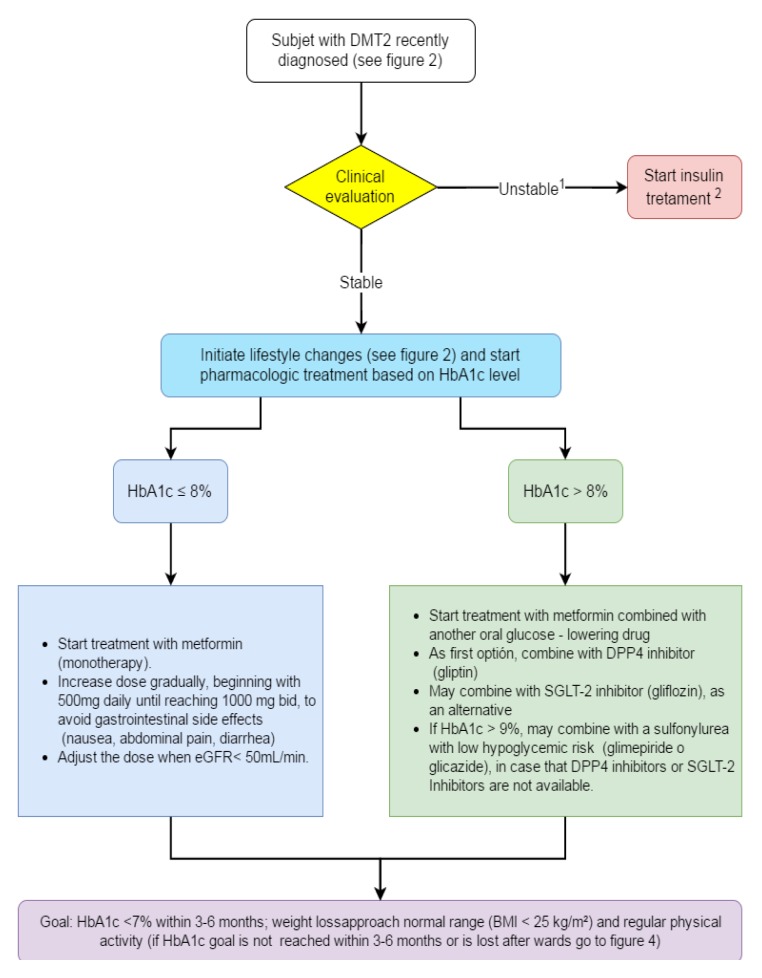
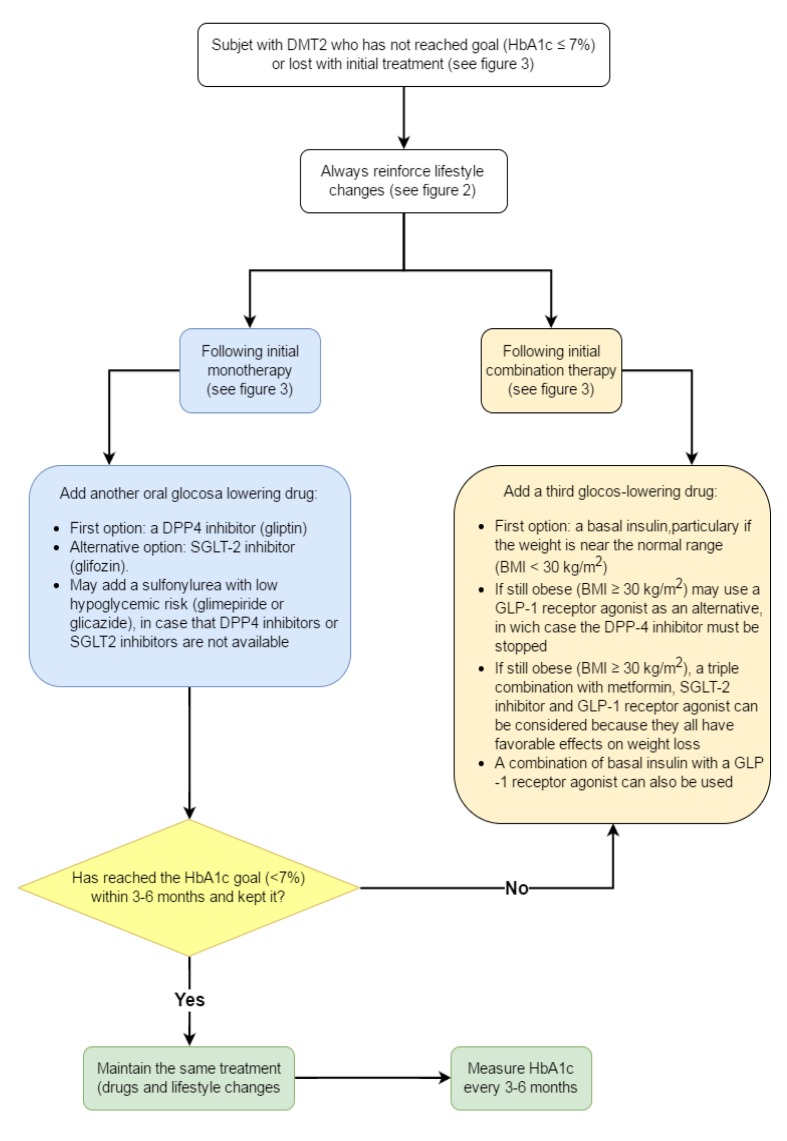
In Colombia, diabetes mellitus is a public health program for those responsible for creating and implementing strategies for prevention, diagnosis, treatment, and follow-up that are applicable at all care levels, with the objective of establishing early and sustained control of diabetes. A clinical practice guide has been developed following the broad outline of the methodological guide from the Ministry of Health and Social Welfare, with the aim of systematically gathering scientific evidence and formulating recommendations using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) methodology. The current document presents in summary form the results of this process, including the recommendations and the considerations taken into account in formulating them. In general terms, what is proposed here is a screening process using the Finnish Diabetes Risk Score questionnaire adapted to the Colombian population, which enables early diagnosis of the illness, and an algorithm for determining initial treatment that can be generalized to most patients with diabetes mellitus type 2 and that is simple to apply in a primary care context. In addition, several recommendations have been made to scale up pharmacological treatment in those patients that do not achieve the objectives or fail to maintain them during initial treatment. These recommendations also take into account the evolution of weight and the individualization of glycemic control goals for special populations. Finally, recommendations have been made for opportune detection of micro- and macrovascular complications of diabetes.
En Colombia la Diabetes Mellitus es un problema de salud pública por lo que deben generarse e implementarse estrategias de prevención, diagnóstico, tratamiento y seguimiento, aplicables en todos los niveles de atención con miras a establecer el control de la diabetes en forma temprana y sostenida. Se elaboró una guía de práctica clínica siguiendo los lineamientos de la guía metodológica del Ministerio de Salud y Protección Social para recolectar de forma sistemática la evidencia científica y formular las recomendaciones utilizando la metodología GRADE. El presente documento muestra, de forma resumida, el resultado de ese proceso, incluyendo las recomendaciones y las consideraciones tenidas en cuenta para llegar a ellas. En términos generales, se propone un proceso de tamización mediante el cuestionario FINDRISC adaptado a población Colombiana que permite llegar a un diagnóstico temprano de la enfermedad y un algoritmo para el manejo inicial que es generalizable a la gran mayoría de los pacientes con diabetes mellitus tipo 2 y que es sencillo de aplicar en atención primaria. También se hacen unas recomendaciones para escalar el tratamiento farmacológico de los pacientes que no alcanzan la meta o la pierden con el manejo inicial, teniendo en cuenta principalmente la evolución del peso y la individualización de la meta de control glucémico en poblaciones especiales. Finalmente se proponen algunas recomendaciones para la detección oportuna de las complicaciones micro y macrovasculares de la diabetes.
Keywords: Type 2 diabetes mellitus; clinical practice guidelines.
Conflict of interest statement
Figures
Similar articles
-
Document on a comprehensive approach to type 2 diabetes mellitus.Endocrinol Diabetes Nutr (Engl Ed). 2019 Aug-Sep;66(7):443-458. doi: 10.1016/j.endinu.2018.10.010. Epub 2019 Feb 28. Endocrinol Diabetes Nutr (Engl Ed). 2019. PMID: 30827909 English, Spanish.
-
Diagnosis and management of type 2 diabetes in adults: a review of the ICSI guideline.Geriatrics. 2009 Jun;64(6):12-7, 29. Geriatrics. 2009. PMID: 19572762
-
Glycated Hemoglobin Level Goal Achievement in Adults With Type 2 Diabetes in Canada: Still Room for Improvement.Can J Diabetes. 2019 Aug;43(6):384-391. doi: 10.1016/j.jcjd.2018.10.005. Epub 2018 Nov 2. Can J Diabetes. 2019. PMID: 30554985
-
Individualizing glycemic targets in type 2 diabetes mellitus: implications of recent clinical trials.Ann Intern Med. 2011 Apr 19;154(8):554-9. doi: 10.7326/0003-4819-154-8-201104190-00007. Ann Intern Med. 2011. PMID: 21502652 Review.
-
Treatment of type 2 diabetes in Latin America: a consensus statement by the medical associations of 17 Latin American countries. Latin American Diabetes Association.Rev Panam Salud Publica. 2010 Dec;28(6):463-71. doi: 10.1590/s1020-49892010001200008. Rev Panam Salud Publica. 2010. PMID: 21308173
Cited by
-
Type 2 diabetes is independently associated with all-cause mortality secondary to ventricular tachyarrhythmias.Cardiovasc Diabetol. 2018 Sep 10;17(1):125. doi: 10.1186/s12933-018-0768-y. Cardiovasc Diabetol. 2018. PMID: 30200967 Free PMC article.
-
Prevalence of the Use of Aspirin and Statins for Preventing Cardiovascular Events in the Colombian Population with Type 2 Diabetes Mellitus: Comparison of 2008 and 2018.J Prim Care Community Health. 2021 Jan-Dec;12:21501327211007015. doi: 10.1177/21501327211007015. J Prim Care Community Health. 2021. PMID: 33787394 Free PMC article.
-
Prediabetes in Colombia: Expert Consensus.Colomb Med (Cali). 2017 Dec 30;48(4):191-203. doi: 10.25100/cm.v43i4.3662. Colomb Med (Cali). 2017. PMID: 29662261 Free PMC article. Review.
-
Reduction in HbA1c with Exercise videogames among participants with elevated HbA1c: Secondary analysis of the Wii Heart Fitness trial.Diabetes Res Clin Pract. 2019 Aug;154:35-42. doi: 10.1016/j.diabres.2019.06.011. Epub 2019 Jun 22. Diabetes Res Clin Pract. 2019. PMID: 31238061 Free PMC article.
-
Severity of Gastrointestinal Side Effects of Metformin Tablet Compared to Metformin Capsule in Type 2 Diabetes Mellitus Patients.J Res Pharm Pract. 2017 Apr-Jun;6(2):73-76. doi: 10.4103/jrpp.JRPP_17_2. J Res Pharm Pract. 2017. PMID: 28616428 Free PMC article.
References
-
- Aschner P. Epidemiología de la diabetes en Colombia. Avances Diabetol. 2010;26:95–100.
-
- Federación Internacional de diabetes . ATLAS de la DIABETES de la FID. 6th. Bruselas, Bélgica: Federación Internacional de Diabetes; 2014.
-
- Aschner PJ, Ruiz AJ. Metabolic memory for vascular disease in diabetes. Diabetes Technol Ther. 2012;14(1):S68–S74. - PubMed
-
- United Kingdom Prospective Diabetes Study Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33) Lancet. 1998;352(9131):837–853. - PubMed
-
- Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HAW. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2008;359(15):1577–1589. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
