

Effect of Fecal Microbiota Transplantation on Recurrence in Multiply Recurrent Clostridium difficile Infection: A Randomized Trial
- PMID: 27547925
- PMCID: PMC5909820
- DOI: 10.7326/M16-0271
Effect of Fecal Microbiota Transplantation on Recurrence in Multiply Recurrent Clostridium difficile Infection: A Randomized Trial
Abstract
Background: To date, evidence for the efficacy of fecal microbiota transplantation (FMT) in recurrent Clostridium difficile infection (CDI) has been limited to case series and open-label clinical trials.
Objective: To determine the efficacy and safety of FMT for treatment of recurrent CDI.
Design: Randomized, controlled, double-blind clinical trial. (ClinicalTrials.gov: NCT01703494).
Setting: Two academic medical centers.
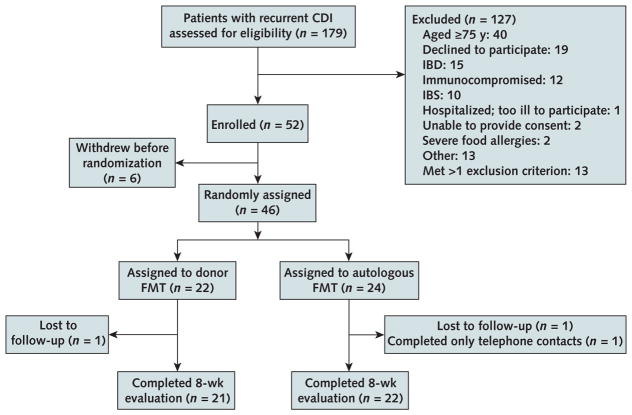
Patients: 46 patients who had 3 or more recurrences of CDI and received a full course of vancomycin for their most recent acute episode.
Intervention: Fecal microbiota transplantation with donor stool (heterologous) or patient's own stool (autologous) administered by colonoscopy.
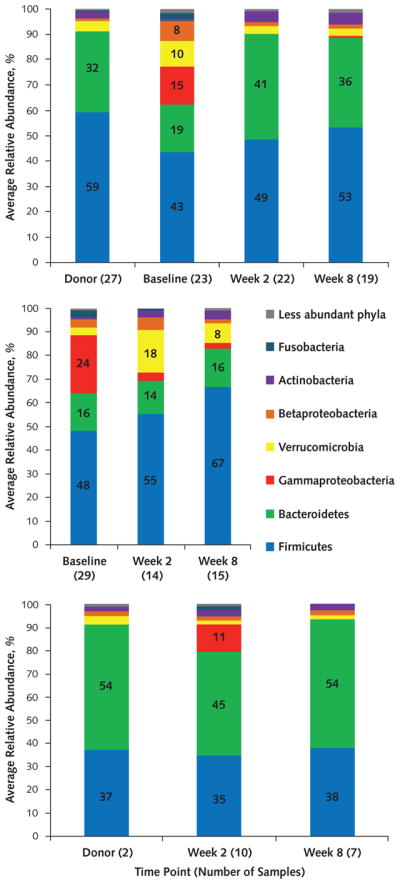
Measurements: The primary end point was resolution of diarrhea without the need for further anti-CDI therapy during the 8-week follow-up. Safety data were compared between treatment groups via review of adverse events (AEs), serious AEs (SAEs), and new medical conditions for 6 months after FMT. Fecal microbiota analyses were performed on patients' stool before and after FMT and also on donors' stool.
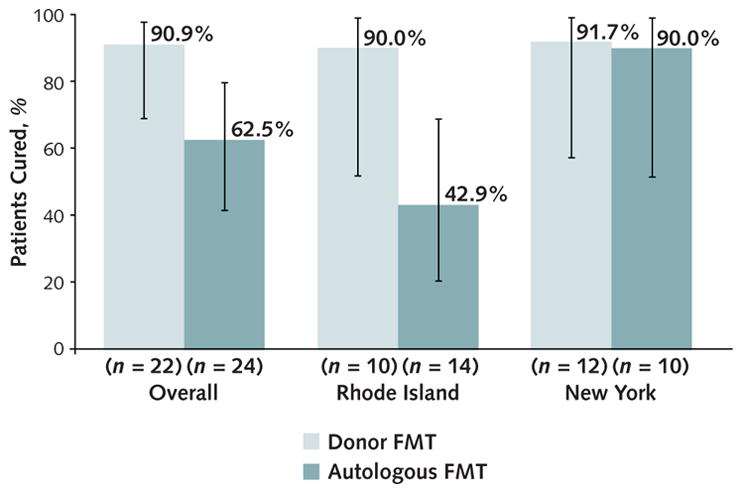
Results: In the intention-to-treat analysis, 20 of 22 patients (90.9%) in the donor FMT group achieved clinical cure compared with 15 of 24 (62.5%) in the autologous FMT group (P = 0.042). Resolution after autologous FMT differed by site (9 of 10 vs. 6 of 14 [P = 0.033]). All 9 patients who developed recurrent CDI after autologous FMT were free of further CDI after subsequent donor FMT. There were no SAEs related to FMT. Donor FMT restored gut bacterial community diversity and composition to resemble that of healthy donors.
Limitation: The study included only patients who had 3 or more recurrences and excluded those who were immunocompromised and aged 75 years or older.
Conclusion: Donor stool administered via colonoscopy seemed safe and was more efficacious than autologous FMT in preventing further CDI episodes.
Primary funding source: National Institute of Diabetes and Digestive and Kidney Diseases.
Figures
Comment in
-
CORR Insights (®) : Higher Pavlik Harness Treatment Failure Is Seen in Graf Type IV Ortolani-Positive Hips in Males.Clin Orthop Relat Res. 2016 Aug;474(8):1855-6. doi: 10.1007/s11999-016-4865-5. Epub 2016 May 6. Clin Orthop Relat Res. 2016. PMID: 27154531 Free PMC article. No abstract available.
-
Are Microbial Politics Local?Ann Intern Med. 2016 Nov 1;165(9):667-668. doi: 10.7326/M16-1784. Epub 2016 Aug 23. Ann Intern Med. 2016. PMID: 27548329 No abstract available.
-
Donor faecal transplantation is highly curative in recurrent C difficile infection, trial finds.BMJ. 2016 Aug 23;354:i4638. doi: 10.1136/bmj.i4638. BMJ. 2016. PMID: 27558248 No abstract available.
References
-
- Cohen SH, Gerding DN, Johnson S, Kelly CP, Loo VG, McDonald LC, et al. Society for Healthcare Epidemiology of America. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA) Infect Control Hosp Epidemiol. 2010;31:431–55. doi: 10.1086/651706. - DOI - PubMed
-
- McFarland LV, Elmer GW, Surawicz CM. Breaking the cycle: treatment strategies for 163 cases of recurrent Clostridium difficile disease. Am J Gastroenterol. 2002;97:1769–75. - PubMed
-
- McFarland LV, Surawicz CM, Rubin M, Fekety R, Elmer GW, Greenberg RN. Recurrent Clostridium difficile disease: epidemiology and clinical characteristics. Infect Control Hosp Epidemiol. 1999;20:43–50. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases