

Color radiography in lung nodule detection and characterization: comparison with conventional gray scale radiography
- PMID: 27549084
- PMCID: PMC4994314
- DOI: 10.1186/s12880-016-0155-7
Color radiography in lung nodule detection and characterization: comparison with conventional gray scale radiography
Abstract
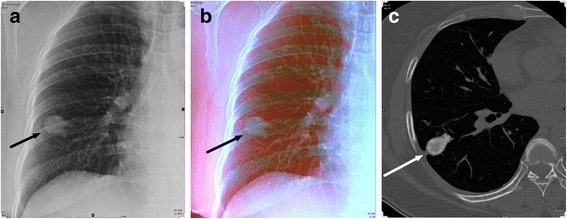
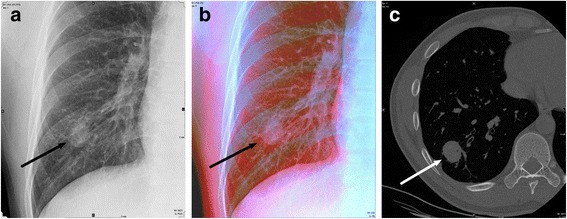
Background: To compare the capability of lung nodule detection and characterization between dual-energy radiography with color-representation (DCR) and conventional gray scale chest radiography (GSR).
Methods: A total of 130 paired chest radiographs (DCR and GSR) obtained from 65 patients (14 with normal scans and 51 with pulmonary nodules) were evaluated. After analysis, 45 non-calcified and 21 calcified nodules were identified. DCR was obtained by adding color space within material-decomposed data (blue for high attenuation and red for low attenuation) and by compounding the manipulated data to one color image. Three radiologists marked suggested nodules on radiographic images and assessed the level of confidence of lesion presence and probability of nodule calcification by using a nine-point rating scale. The jackknife active free-response receiver operating characteristics (JAFROC) analysis was used to evaluate lesion detectability, and multi-reader multi-case receiver operating characteristics (MRMC ROC) analysis was used for the evaluation of the accuracy of nodule calcification prediction.
Results: Figures of merit (FOM) from JAFROC was 0.807 for DCR and 0.811 for GSR, respectively; nodule detectability was not significantly different between DCR and GSR (p = 0.93). Areas under curve (AUC) from MRMC ROC were 0.944 for DCR and 0.828 for GSR, respectively; performance of DCR in predicting lung nodule calcification was significantly higher than that of GSR (p = 0.04).
Conclusions: DCR showed similar performance in terms of lung nodule detection compared with GSR. However, DCR does provide a significant benefit in predicting the presence of nodule calcification.
Keywords: Color radiography; Dual-energy subtraction radiography; Radiography.
Figures

Similar articles
-
Conventional chest radiography vs dual-energy computed radiography in the detection and characterization of pulmonary nodules.AJR Am J Roentgenol. 1994 Feb;162(2):271-8. doi: 10.2214/ajr.162.2.8310908. AJR Am J Roentgenol. 1994. PMID: 8310908
-
Comparison of dual-energy subtraction and electronic bone suppression combined with computer-aided detection on chest radiographs: effect on human observers' performance in nodule detection.AJR Am J Roentgenol. 2013 May;200(5):1006-13. doi: 10.2214/AJR.12.8877. AJR Am J Roentgenol. 2013. PMID: 23617482 Clinical Trial.
-
Role of digital tomosynthesis and dual energy subtraction digital radiography in detecting pulmonary nodules.Eur J Radiol. 2015 Jul;84(7):1383-91. doi: 10.1016/j.ejrad.2015.03.020. Epub 2015 Mar 24. Eur J Radiol. 2015. PMID: 25892052
-
Dual energy subtraction digital radiography: technical considerations, clinical applications, and imaging pitfalls.J Thorac Imaging. 2006 Nov;21(4):303-13. doi: 10.1097/01.rti.0000213646.34417.be. J Thorac Imaging. 2006. PMID: 17110857 Review.
-
[Paradigm Shift in Respiratory Diagnosis: Current Status and Future Prospects of Dynamic Chest Radiography].Nihon Hoshasen Gijutsu Gakkai Zasshi. 2021;77(11):1279-1287. doi: 10.6009/jjrt.2021_JSRT_77.11.1279. Nihon Hoshasen Gijutsu Gakkai Zasshi. 2021. PMID: 34803108 Review. Japanese.
Cited by
-
The detection of lung cancer using massive artificial neural network based on soft tissue technique.BMC Med Inform Decis Mak. 2020 Oct 31;20(1):282. doi: 10.1186/s12911-020-01220-z. BMC Med Inform Decis Mak. 2020. PMID: 33129343 Free PMC article.
References
-
- Henschke CI, McCauley DI, Yankelevitz DF, Naidich DP, McGuinness G, Miettinen OS, Libby DM, Pasmantier MW, Koizumi J, Altorki NK, et al. Early Lung Cancer Action Project: overall design and findings from baseline screening. Lancet. 1999;354(9173):99–105. doi: 10.1016/S0140-6736(99)06093-6. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
