

Impact of electronic medication reconciliation interventions on medication discrepancies at hospital transitions: a systematic review and meta-analysis
- PMID: 27549581
- PMCID: PMC4994239
- DOI: 10.1186/s12911-016-0353-9
Impact of electronic medication reconciliation interventions on medication discrepancies at hospital transitions: a systematic review and meta-analysis
Abstract
Background: Medication reconciliation has been identified as an important intervention to minimize the incidence of unintentional medication discrepancies at transitions in care. However, there is a lack of evidence for the impact of information technology on the rate and incidence of medication discrepancies identified during care transitions. This systematic review was thus, aimed to evaluate the impact of electronic medication reconciliation interventions on the occurrence of medication discrepancies at hospital transitions.
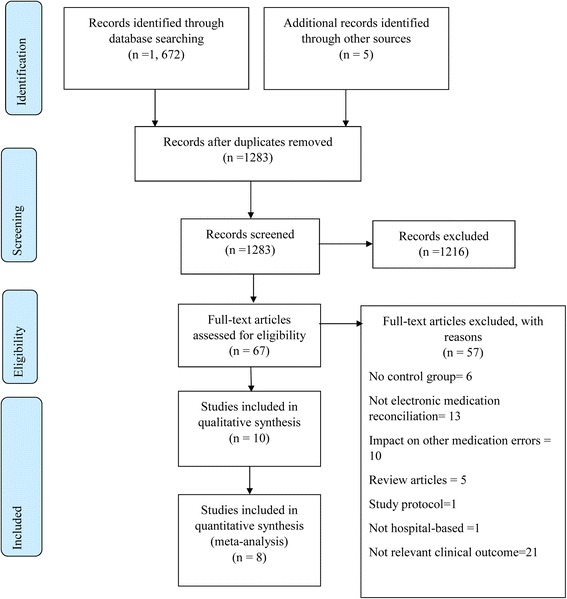
Methods: Systematic literature searches were performed in MEDLINE, PubMed, CINHAL, and EMBASE from inception to November, 2015. We included published studies in English that evaluated the effect of information technology on the incidence and rate of medication discrepancies compared with usual care. Cochrane's tools were used for assessment of the quality of included studies. We performed meta-analyses using random-effects models.
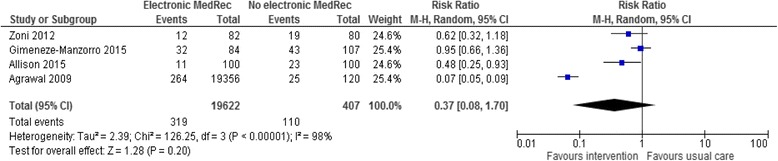
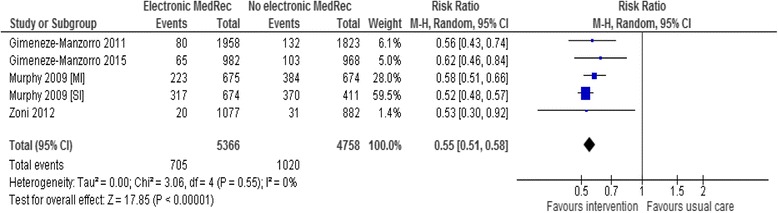
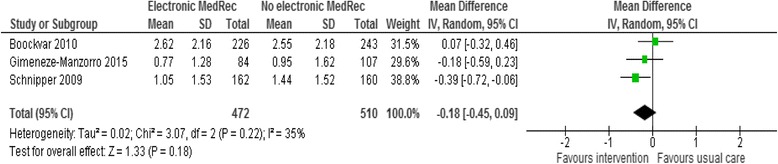
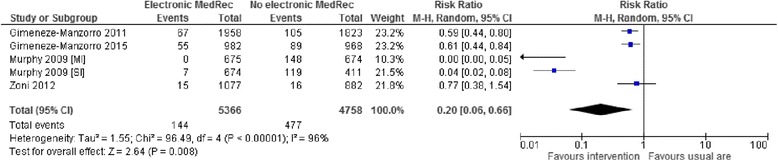
Results: Ten studies met our inclusion criteria; of which only one was a randomized controlled trial. Interventions were carried out at various hospital transitions (admission, 5; discharge, 2 and multiple transitions, 3 studies). Meta-analysis showed a significant reduction of 45 % in the proportion of medications with unintentional discrepancies after the use of electronic medication reconciliation (RR 0.55; 95 % CI 0.51 to 0.58). However, there was no significant reduction in either the proportion of patients with medication discrepancies or the mean number of discrepancies per patient. Drug omissions were the most common types of unintended discrepancies, and with an electronic tool a significant but heterogeneously distributed reduction of omission errors over the total number of medications reconciled have been observed (RR 0.20; 95 % CI 0.06 to 0.66). The clinical impact of unintended discrepancies was evaluated in five studies, and there was no potentially fatal error identified and most errors were minor in severity.
Conclusion: Medication reconciliation supported by an electronic tool was able to minimize the incidence of medications with unintended discrepancy, mainly drug omissions. But, this did not consistently reduce other process outcomes, although there was a lack of rigorous design to conform these results.
Keywords: Care transition; Electronic medication reconciliation; Medication discrepancies; Medication errors; Medication history; Medication safety.
Figures
References
-
- Joint Commission on Accreditation for Healthcare Organizations. National Patient Safety Goals. 2006. Available at: https://www.jointcommission.org/improving_americas_hospitals_the_joint_c.... Accessed 30 Jan 2016.
-
- National Institute for Health and Care Excellence. Medicines optimisation: the safe and effective use of medicines to enable the best possible outcomes. NICE guideline, March 2015. Available at: https://www.nice.org.uk/guidance/ng5. Accessed 30 Jan 2016. - PubMed
-
- Accreditation Canada. Required organizational practices handbook. 2016. Ottawa, Available at: https://accreditation.ca/sites/default/files/rop-handbook-2016-en.pdf. Accessed 30 Jan 2016.
-
- Australian Commission on Safety and Quality in Healthcare. Medication reconciliation. Avialable at: http://www.safetyandquality.gov.au/our-work/medication-safety/medication.... Accessed 30 Jan 2016.
-
- Rozich JD, Howard RJ, Justeson JM, Macken PD, Lindsay ME, Resar RK. Standardization as a mechanism to improve safety in health care. Jt Comm J Qual Saf. 2004;30(1):5–14. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
