

Metastatic Breast Cancer With ESR1 Mutation: Clinical Management Considerations From the Molecular and Precision Medicine (MAP) Tumor Board at Massachusetts General Hospital
- PMID: 27551012
- PMCID: PMC5016066
- DOI: 10.1634/theoncologist.2016-0240
Metastatic Breast Cancer With ESR1 Mutation: Clinical Management Considerations From the Molecular and Precision Medicine (MAP) Tumor Board at Massachusetts General Hospital
Abstract
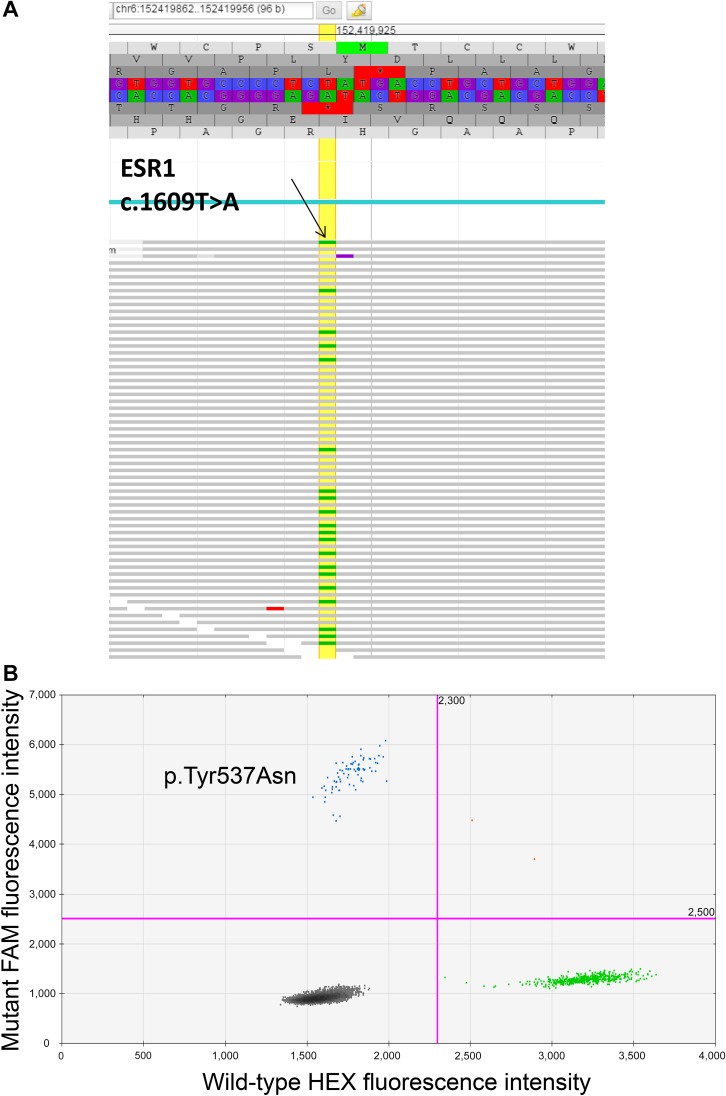
: The last decade in oncology has witnessed impressive response rates with targeted therapies, largely because of collaborative efforts at understanding tumor biology and careful patient selection based on molecular fingerprinting of the tumor. Consequently, there has been a push toward routine molecular genotyping of tumors, and large precision medicine-based clinical trials have been launched to match therapy to the molecular alteration seen in a tumor. However, selecting the "right drug" for an individual patient in clinic is a complex decision-making process, including analytical interpretation of the report, consideration of the importance of the molecular alteration in driving growth of the tumor, tumor heterogeneity, the availability of a matched targeted therapy, efficacy and toxicity considerations of the targeted therapy (compared with standard therapy), and reimbursement issues. In this article, we review the key considerations involved in clinical decision making while reviewing a molecular genotyping report. We present the case of a 67-year-old postmenopausal female with metastatic estrogen receptor-positive (ER+) breast cancer, whose tumor progressed on multiple endocrine therapies. Molecular genotyping of the metastatic lesion revealed the presence of an ESR1 mutation (encoding p.Tyr537Asn), which was absent in the primary tumor. The same ESR1 mutation was also detected in circulating tumor DNA (ctDNA) extracted from her blood. The general approach for interpretation of genotyping results, the clinical significance of the specific mutation in the particular cancer, potential strategies to target the pathway, and implications for clinical practice are reviewed in this article.
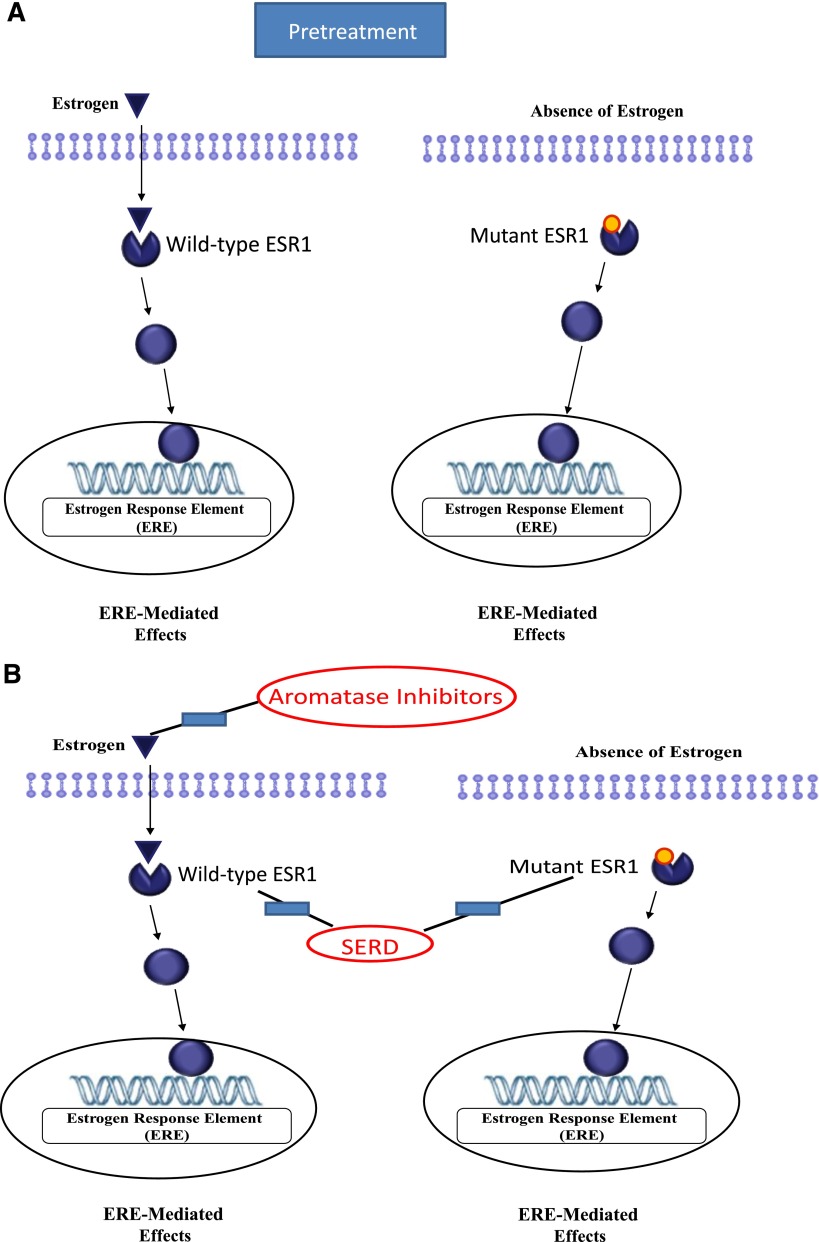
Key points: ER+ breast tumors are known to undergo genomic evolution during treatment with the acquisition of new mutations that confer resistance to treatment.ESR1 mutations in the ligand-binding domain of ER can lead to a ligand-independent, constitutively active form of ER and mediate resistance to aromatase inhibitors.ESR1 mutations may be detected by genomic sequencing of tissue biopsies of the metastatic tumor or by sequencing the circulating tumor cells or tumor DNA (ctDNA).Sequencing results may lead to a therapeutic "match" with an existing FDA-approved drug or match with an experimental agent that fits the clinical setting.
摘要
肿瘤学在过去十年里见证了靶向疗法惊人的缓解率, 这很大程度上是缘于对肿瘤生物学的深入理解和基于肿瘤分子指纹图谱对患者进行仔细选择的通力协作。继而, 肿瘤分子基因分型的常规检测得到推动, 研究者开展了大量以精确医学为基础的临床试验以匹配治疗与肿瘤中的分子改变。但是在临床上为一名患者选择“正确的药物”是一个复杂的决策制定过程, 包括对报告进行分析性解读、考虑分子改变在驱动肿瘤生长中的重要性、肿瘤异质性、可用的匹配靶向治疗、靶向治疗的有效性和安全性考量 (与标准治疗相比) 以及费用报销问题。作者在本文中回顾了一个分子基因分型案例报告, 同时综述了临床决策制定过程中涉及的关键问题。该案例为一名罹患雌激素受体阳性 (ER+) 乳腺癌的67岁绝经后女性, 在接受多种内分泌治疗后肿瘤出现进展。转移灶的分子基因分型提示存在ESR1突变 (编码p.Tyr537Asn), 而原发肿瘤中不存在该突变。从血中提取的循环肿瘤DNA (ctDNA) 中也检测到同样的ESR1突变。本文对基因分型结果的一般解释方法、特定肿瘤中特异性突变的临床意义、针对通路进行干预的可能策略以及对临床实践的提示进行了综述。The Oncologist 2016;21:1035–1040
关键点
• 已知 ER+乳腺肿瘤在治疗过程中会发生基因组演变, 获得使肿瘤对治疗产生耐药的新突变。
• ER 配体结合域的 ESR1 突变可导致 ER 发生非配体依赖的结构活性, 介导芳香化酶抑制剂耐药的发生。
• 对转移肿瘤的组织活检标本进行基因组测序, 或者对循环肿瘤细胞或肿瘤 DNA (ctDNA) 进行测序, 可能检测到 ESR1 突变。
• 测序结果也许能够找到“匹配”的现有 FDA 批准的药物或者适用于临床环境的实验性制剂。
©AlphaMed Press.
Conflict of interest statement
of potential conflicts of interest may be found at the end of this article.
Figures
Similar articles
-
Short report: Monitoring ESR1 mutations by circulating tumor DNA in aromatase inhibitor resistant metastatic breast cancer.Int J Cancer. 2015 Nov 15;137(10):2513-9. doi: 10.1002/ijc.29612. Epub 2015 Jun 11. Int J Cancer. 2015. PMID: 25994408
-
The Evolving Role of the Estrogen Receptor Mutations in Endocrine Therapy-Resistant Breast Cancer.Curr Oncol Rep. 2017 May;19(5):35. doi: 10.1007/s11912-017-0591-8. Curr Oncol Rep. 2017. PMID: 28374222 Review.
-
Evaluation of endocrine resistance using ESR1 genotyping of circulating tumor cells and plasma DNA.Breast Cancer Res Treat. 2021 Jul;188(1):43-52. doi: 10.1007/s10549-021-06270-z. Epub 2021 Jun 8. Breast Cancer Res Treat. 2021. PMID: 34101078 Free PMC article.
-
Tracking evolution of aromatase inhibitor resistance with circulating tumour DNA analysis in metastatic breast cancer.Ann Oncol. 2018 Jan 1;29(1):145-153. doi: 10.1093/annonc/mdx483. Ann Oncol. 2018. PMID: 29045530 Free PMC article.
-
ESR1 mutation as an emerging clinical biomarker in metastatic hormone receptor-positive breast cancer.Breast Cancer Res. 2021 Aug 15;23(1):85. doi: 10.1186/s13058-021-01462-3. Breast Cancer Res. 2021. PMID: 34392831 Free PMC article. Review.
Cited by
-
Genomic Landscape of Uterine Sarcomas Defined Through Prospective Clinical Sequencing.Clin Cancer Res. 2020 Jul 15;26(14):3881-3888. doi: 10.1158/1078-0432.CCR-19-3959. Epub 2020 Apr 16. Clin Cancer Res. 2020. PMID: 32299819 Free PMC article.
-
Development, Validation, and Dissemination of a Breast Cancer Recurrence Detection and Timing Informatics Algorithm.J Natl Cancer Inst. 2018 Mar 1;110(3):273-281. doi: 10.1093/jnci/djx200. J Natl Cancer Inst. 2018. PMID: 29873757 Free PMC article.
-
Precision Oncology Decision Support: Current Approaches and Strategies for the Future.Clin Cancer Res. 2018 Jun 15;24(12):2719-2731. doi: 10.1158/1078-0432.CCR-17-2494. Epub 2018 Feb 2. Clin Cancer Res. 2018. PMID: 29420224 Free PMC article. Review.
-
Estrogen-Receptor Loss and ESR1 Mutation in Estrogen-Receptor-Positive Metastatic Breast Cancer and the Effect on Overall Survival.Cancers (Basel). 2024 Aug 30;16(17):3025. doi: 10.3390/cancers16173025. Cancers (Basel). 2024. PMID: 39272884 Free PMC article.
-
Performance of Cancer Recurrence Algorithms After Coding Scheme Switch From International Classification of Diseases 9th Revision to International Classification of Diseases 10th Revision.JCO Clin Cancer Inform. 2019 Mar;3:1-9. doi: 10.1200/CCI.18.00113. JCO Clin Cancer Inform. 2019. PMID: 30869998 Free PMC article.
References
-
- McCarthy M. US president endorses “moonshot” effort to cure cancer. BMJ. 2016;352:i213. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
