

Cost-Effectiveness Analysis of Elective Neck Dissection in Patients With Clinically Node-Negative Oral Cavity Cancer
- PMID: 27551113
- PMCID: PMC5457359
- DOI: 10.1200/JCO.2016.68.4563
Cost-Effectiveness Analysis of Elective Neck Dissection in Patients With Clinically Node-Negative Oral Cavity Cancer
Abstract
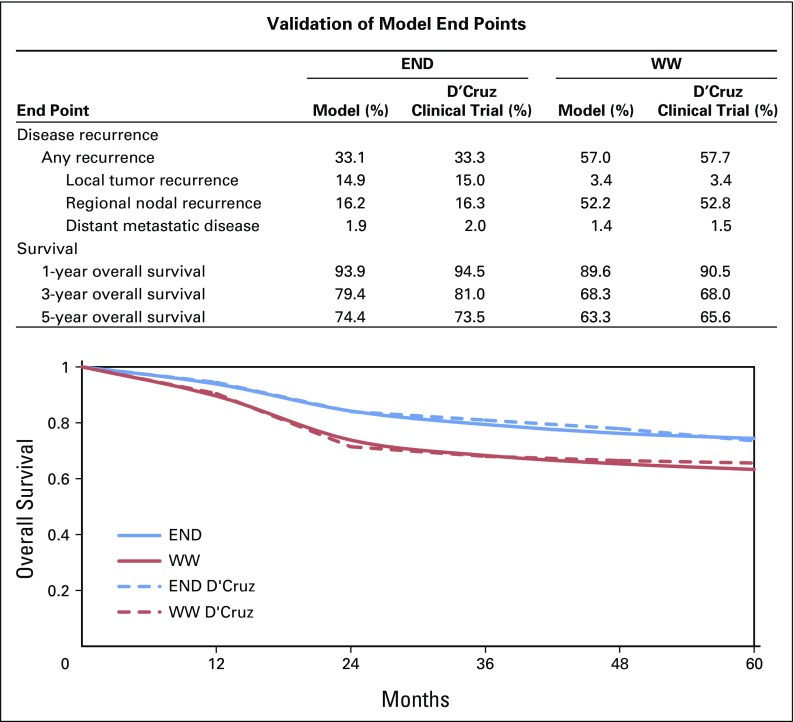
Purpose Recently, a large randomized trial found a survival advantage among patients who received elective neck dissection in conjunction with primary surgery for clinically node-negative oral cavity cancer compared with those receiving primary surgery alone. However, elective neck dissection comes with greater upfront cost and patient morbidity. We present a cost-effectiveness analysis of elective neck dissection for the initial surgical management of early-stage oral cavity cancer. Methods We constructed a Markov model to simulate primary, adjuvant, and salvage therapy; disease recurrence; and survival in patients with T1/T2 clinically node-negative oral cavity squamous cell carcinoma. Transition probabilities were derived from clinical trial data; costs (in 2015 US dollars) and health utilities were estimated from the literature. Incremental cost-effectiveness ratios, expressed as dollar per quality-adjusted life-year (QALY), were calculated with incremental cost-effectiveness ratios less than $100,000/QALY considered cost effective. We conducted one-way and probabilistic sensitivity analyses to examine model uncertainty. Results Our base-case model found that over a lifetime the addition of elective neck dissection to primary surgery reduced overall costs by $6,000 and improved effectiveness by 0.42 QALYs compared with primary surgery alone. The decrease in overall cost despite the added neck dissection was a result of less use of salvage therapy. On one-way sensitivity analysis, the model was most sensitive to assumptions about disease recurrence, survival, and the health utility reduction from a neck dissection. Probabilistic sensitivity analysis found that treatment with elective neck dissection was cost effective 76% of the time at a willingness-to-pay threshold of $100,000/QALY. Conclusion Our study found that the addition of elective neck dissection reduces costs and improves health outcomes, making this a cost-effective treatment strategy for patients with early-stage oral cavity cancer.
Conflict of interest statement
Authors’ disclosures of potential conflicts of interest are found in the article online at
Figures




References
-
- Ferlay J, Soerjomataram I, Ervik M, et al: GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase. No. 11 [Internet]. Lyon, France: International Agency for Research on Cancer; 2013. http://globocan.iarc.fr.
-
- Haddadin KJ, Soutar DS, Oliver RJ, et al: Improved survival for patients with clinically T1/T2, N0 tongue tumors undergoing a prophylactic neck dissection. Head Neck 21:517-525, 1999. - PubMed
-
- Greenberg JS, El Naggar AK, Mo V, et al. Disparity in pathologic and clinical lymph node staging in oral tongue carcinoma. Implication for therapeutic decision making. Cancer. 2003;98:508–515. - PubMed
-
- D’Cruz AK, Vaish R, Kapre N, et al. Elective versus therapeutic neck dissection in node-negative oral cancer. N Engl J Med. 2015;373:521–529. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
