

Obesity and Airway Dysanapsis in Children with and without Asthma
- PMID: 27552676
- PMCID: PMC5328183
- DOI: 10.1164/rccm.201605-1039OC
Obesity and Airway Dysanapsis in Children with and without Asthma
Abstract
Rationale: For unclear reasons, obese children with asthma have higher morbidity and reduced response to inhaled corticosteroids.
Objectives: To assess whether childhood obesity is associated with airway dysanapsis (an incongruence between the growth of the lungs and the airways) and whether dysanapsis is associated with asthma morbidity.
Methods: We examined the relationship between obesity and dysanapsis in six cohorts of children with and without asthma, as well as the relationship between dysanapsis and clinical outcomes in children with asthma. Adjusted odds ratios (ORs) were calculated for each cohort and in a combined analysis of all cohorts; longitudinal analyses were also performed for cohorts with available data. Hazard ratios (HRs) for clinical outcomes were calculated for children with asthma in the Childhood Asthma Management Program.
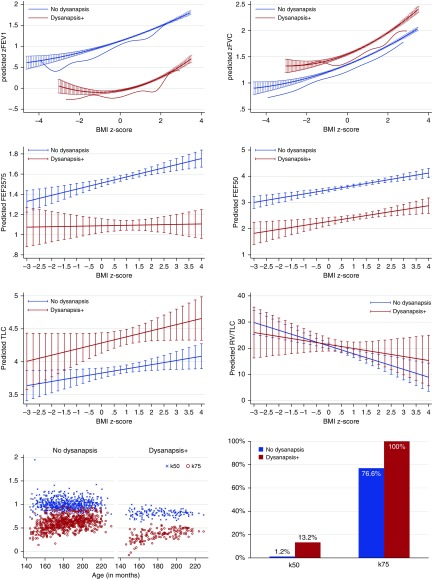
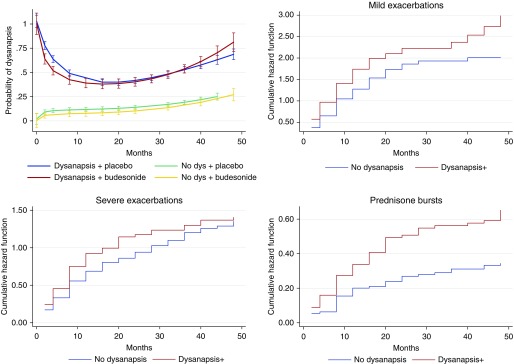
Measurements and main results: Being overweight or obese was associated with dysanapsis in both the cross-sectional (OR, 1.95; 95% confidence interval [CI], 1.62-2.35 [for overweight/obese compared with normal weight children]) and the longitudinal (OR, 4.31; 95% CI, 2.99-6.22 [for children who were overweight/obese at all visits compared with normal weight children]) analyses. Dysanapsis was associated with greater lung volumes (FVC, vital capacity, and total lung capacity) and lesser flows (FEV1 and forced expiratory flow, midexpiratory phase), and with indicators of ventilation inhomogeneity and anisotropic lung and airway growth. Among overweight/obese children with asthma, dysanapsis was associated with severe disease exacerbations (HR, 1.95; 95% CI, 1.38-2.75) and use of systemic steroids (HR, 3.22; 95% CI, 2.02-5.14).
Conclusions: Obesity is associated with airway dysanapsis in children. Dysanapsis is associated with increased morbidity among obese children with asthma and may partly explain their reduced response to inhaled corticosteroids.
Keywords: airway dysanapsis; childhood asthma; childhood obesity; pulmonary function.
Figures
Comment in
-
Dysanapsis-Once Believed to be a Physiological Curiosity-Is Now Clinically Important.Am J Respir Crit Care Med. 2017 Feb 1;195(3):277-278. doi: 10.1164/rccm.201609-1959ED. Am J Respir Crit Care Med. 2017. PMID: 28145760 No abstract available.
References
-
- Dixon AE, Holguin F, Sood A, Salome CM, Pratley RE, Beuther DA, Celedón JC, Shore SA American Thoracic Society Ad Hoc Subcommittee on Obesity and Lung Disease. An official American Thoracic Society Workshop report: obesity and asthma. Proc Am Thorac Soc. 2010;7:325–335. - PubMed
-
- Dixon AE, Pratley RE, Forgione PM, Kaminsky DA, Whittaker-Leclair LA, Griffes LA, Garudathri J, Raymond D, Poynter ME, Bunn JY, et al. Effects of obesity and bariatric surgery on airway hyperresponsiveness, asthma control, and inflammation. J Allergy Clin Immunol. 2011;128:508–515.e1–515.e2. - PMC - PubMed
-
- Jones RL, Nzekwu MM. The effects of body mass index on lung volumes. Chest. 2006;130:827–833. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
