

Comparative effectiveness of levetiracetam, valproate and carbamazepine among elderly patients with newly diagnosed epilepsy: subgroup analysis of the randomized, unblinded KOMET study
- PMID: 27552848
- PMCID: PMC4995751
- DOI: 10.1186/s12883-016-0663-7
Comparative effectiveness of levetiracetam, valproate and carbamazepine among elderly patients with newly diagnosed epilepsy: subgroup analysis of the randomized, unblinded KOMET study
Abstract
Background: Few clinical trials have evaluated the efficacy and tolerability of antiepileptic drugs (AEDs) as initial monotherapy for elderly patients.
Methods: This post-hoc subgroup analysis of data from an unblinded, randomized, 52-week superiority study (KOMET) compared the effectiveness of levetiracetam (LEV) with extended-release sodium valproate (VPA-ER) and controlled-release carbamazepine (CBZ-CR) as monotherapy in patients aged ≥ 60 years with newly diagnosed epilepsy. The physician chose VPA or CBZ as preferred standard treatment; patients were randomized to standard AEDs or LEV. The primary endpoint was time to treatment withdrawal. Results are exploratory, since KOMET was not powered for a subgroup analysis by age.
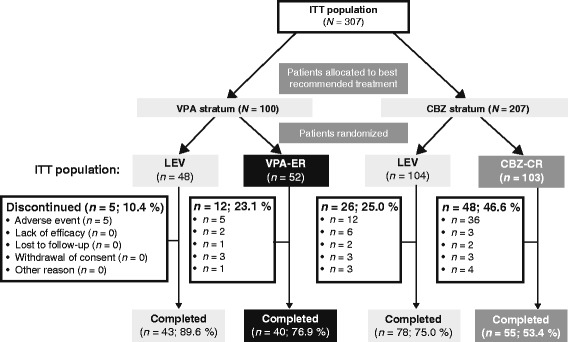
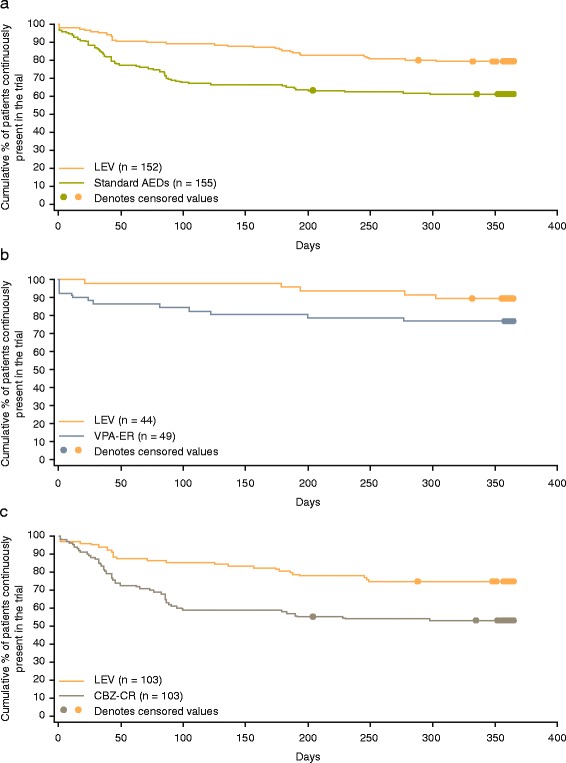
Results: Patients (n = 308) were randomized to LEV (n = 48) or VPA-ER (n = 53) in the VPE-ER stratum or to LEV (n = 104) or CBZ-CR (n = 103) in the CBZ-CR stratum. Mean age was 69.6 years, range 60.2-89.9 years (intention-to-treat population n = 307). Time to treatment withdrawal hazard ratio [HR] (95 % confidence interval [CI]) for LEV vs. standard AEDs was 0.44 (0.28-0.67); LEV vs.
Vpa-er: 0.46 (0.16-1.33); LEV vs.
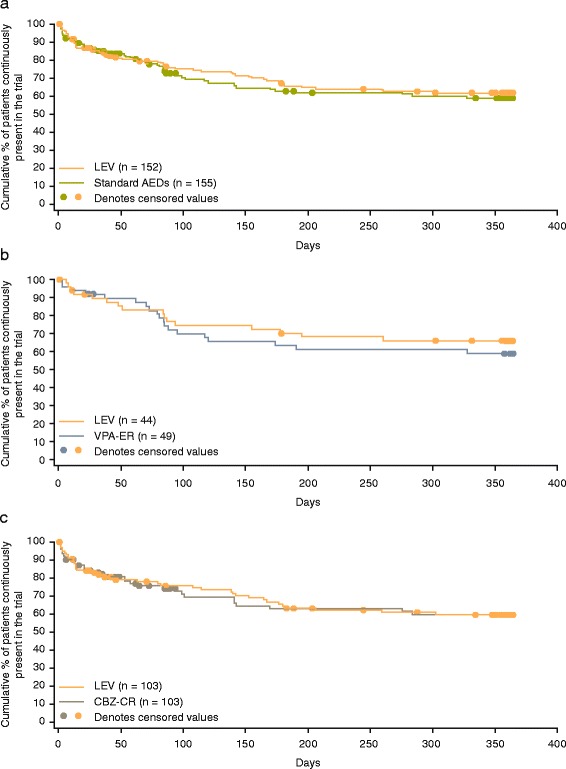
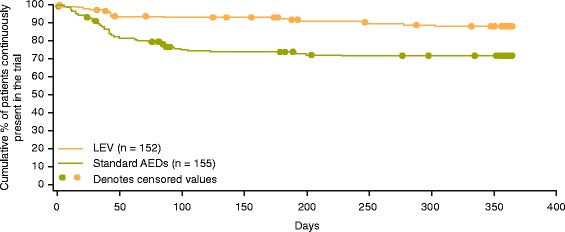
Cbz-cr: 0.45 (0.28-0.72). Twelve-month withdrawal rates were: LEV vs. standard AEDs, 20.4 vs. 38.7 %; LEV vs. VPA-ER, 10.4 vs. 23.1 %; LEV vs. CBZ-CR, 25.0 vs. 46.6 %. Time to first seizure was similar between LEV and standard AEDs (HR: 0.92, 95 % CI: 0.63-1.35), LEV and VPA-ER (0.77, 0.38-1.56), and LEV and CBZ-CR (1.02, 0.64-1.63). Adverse events were reported by 76.2, 67.3, and 82.5 % of patients for LEV, VPA-ER, and CBZ-CR, respectively. Discontinuation rates due to AEs were 11.3, 10.2, and 35.0 % for LEV, VPA-ER, and CBZ-CR, respectively.
Conclusions: Time to treatment withdrawal was longer with LEV compared with standard AEDs. This finding was driven primarly by the result in the CBZ-CR stratum, which in turn was likely due to the more favorable tolerability profile of LEV. Results of this post-hoc analysis suggest that LEV may be a suitable option for initial monotherapy for patients aged ≥ 60 years with newly diagnosed epilepsy.
Trial registration: ClinicalTrials.gov: NCT00175903 ; September 9, 2005.
Keywords: Antiepileptic drug; Elderly; Epilepsy; Levetiracetam; Monotherapy.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
