

Early prediction of outcome after severe traumatic brain injury: a simple and practical model
- PMID: 27553436
- PMCID: PMC4995825
- DOI: 10.1186/s12873-016-0098-x
Early prediction of outcome after severe traumatic brain injury: a simple and practical model
Abstract
Background: Traumatic brain injury (TBI) is a heterogeneous syndrome with a broad range of outcome. We developed a simple model for long-term outcome prognostication after severe TBI.
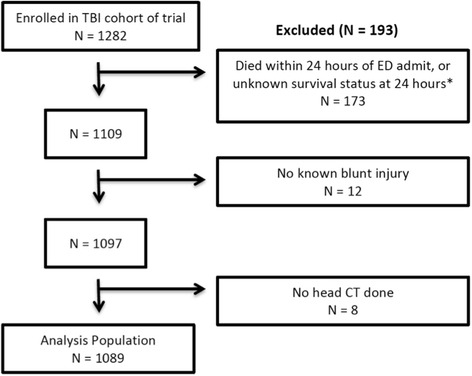
Methods: Secondary data analysis of a large multicenter randomized trial. Patients were grouped according to 6-month extended Glasgow outcome scale (eGOS): poor-outcome (eGOS ≤ 4; severe disability or death) and acceptable outcome (eGOS > 4; no or moderate disability). A prediction decision tree was built using binary recursive partitioning to predict poor or acceptable 6-month outcome. Comparison to two previously published and validated models was made.
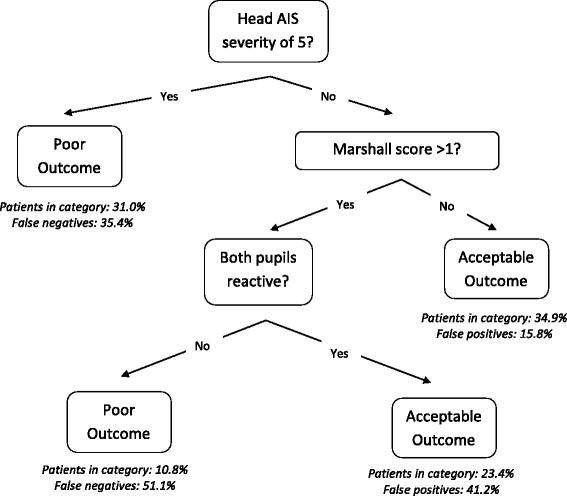
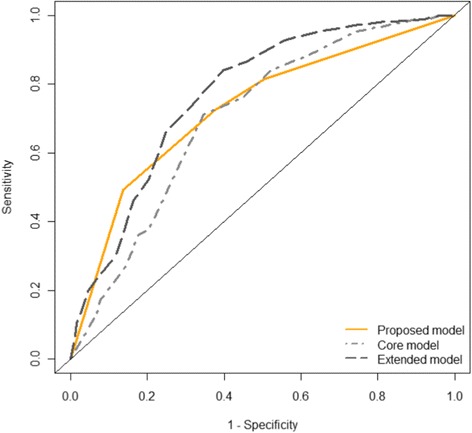
Results: The decision tree included the predictors of head Abbreviated Injury Scale (AIS) severity, the Marshall computed tomography score, and pupillary reactivity. All patients with a head AIS severity of 5 were predicted to have a poor outcome. In patients with head AIS severity < 5, the model predicted an acceptable outcome for (1) those with Marshall score of 1, and (2) those with Marshall score above 1 but with reactive pupils at admission. The decision tree had a sensitivity of 72.3 % (95 % CI: 66.4-77.6 %) and specificity of 62.5 % (95 % CI: 54.9-69.6 %). The proportion correctly classified for the comparison models was similar to our model. Our model was more apt at correctly classifying those with poor outcome but more likely to misclassify those with acceptable outcome than the comparison models.
Conclusion: Predicting long-term outcome early after TBI remains challenging and inexact. This model could be useful for research and quality improvement studies to provide an early assessment of injury severity, but is not sufficiently accurate to guide decision-making in the clinical setting.
Keywords: Outcome measures; Prognostic models; Recovery; Traumatic brain injury.
Figures
References
-
- Bulger EM, May S, Brasel KJ, Schreiber M, Kerby JD, Tisherman SA, Newgard C, Slutsky A, Coimbra R, Emerson S, Minei JP, Bardarson B, Kudenchuk P, Baker A, Christenson J, Idris A, Davis D, Fabian TC, Aufderheide TP, Callaway C, Williams C, Banek J, Vaillancourt C, van Heest R, Sopko G, Hata JS, Hoyt DB, ROC Investigators Out-of-hospital hypertonic resuscitation following severe traumatic brain injury: a randomized controlled trial. JAMA. 2010;304:1455–1464. doi: 10.1001/jama.2010.1405. - DOI - PMC - PubMed
-
- MRC CRASH Trial Collaborators. Perel P, Arango M, Clayton T, Edwards P, Komolafe E, Poccock S, Roberts I, Shakur H, Steyerberg E, Yutthakasemsunt S. Predicting outcome after traumatic brain injury: practical prognostic models based on large cohort of international patients. BMJ. 2008;336:425–429. doi: 10.1136/bmj.39461.643438.25. - DOI - PMC - PubMed
-
- Thompson K, Antony A, Holtzman A. The costs of traumatic brain injury. NC Med J. 2001;62:376–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
