

Glycemic Control for Patients With Type 2 Diabetes Mellitus: Our Evolving Faith in the Face of Evidence
- PMID: 27553599
- PMCID: PMC5031530
- DOI: 10.1161/CIRCOUTCOMES.116.002901
Glycemic Control for Patients With Type 2 Diabetes Mellitus: Our Evolving Faith in the Face of Evidence
Abstract
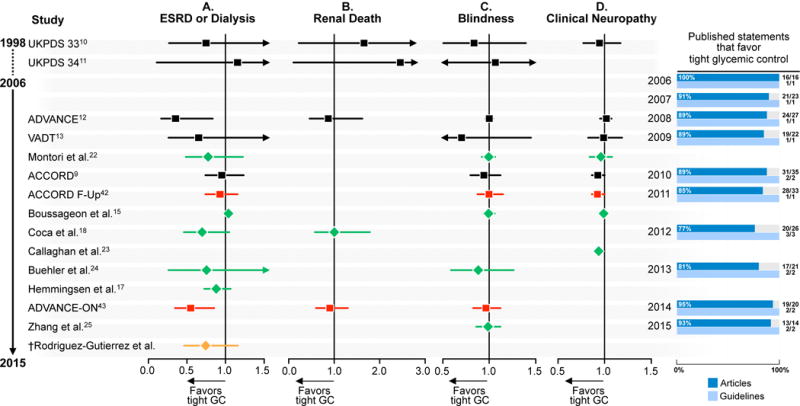
Background: We sought to determine the concordance between the accumulating evidence about the impact of tight versus less tight glycemic control in patients with type 2 diabetes mellitus since the publication of UKPDS (UK Prospective Diabetes Study) in 1998 until 2015 with the views about that evidence published in journal articles and practice guidelines.
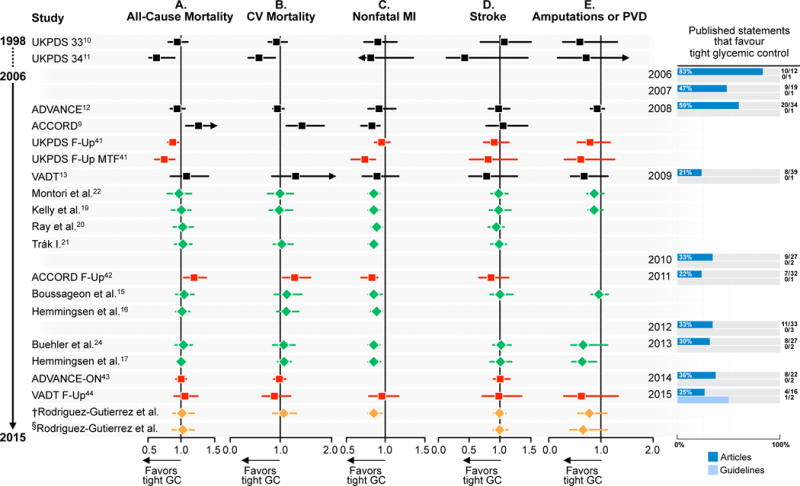
Methods and results: We searched in top general medicine and specialty journals for articles referring to glycemic control appearing between 2006 and 2015 and identified the latest practice guidelines. To summarize the evidence, we included all published systematic reviews and meta-analyses of contemporary randomized trials of glycemic control measuring patient-important microvascular and macrovascular outcomes, and completed a meta-analysis of their follow-up extensions. We identified 16 guidelines and 328 statements. The body of evidence produced estimates warranting moderate confidence. This evidence reported no significant impact of tight glycemic control on the risk of dialysis/transplantation/renal death, blindness, or neuropathy. In the past decade, however, most published statements (77%-100%) and guidelines (95%) unequivocally endorsed benefit. There is also no significant effect on all-cause mortality, cardiovascular mortality, or stroke; however, there is a consistent 15% relative-risk reduction of nonfatal myocardial infarction. Between 2006 and 2008, most statements (47%-83%) endorsed the benefit; after 2008 (ACCORD), only a minority (21%-36%) did.
Conclusions: Discordance exists between the research evidence and academic and clinical policy statements about the value of tight glycemic control to reduce micro- and macrovascular complications. This discordance may distort priorities in the research and practice agendas designed to improve the lives of patients with type 2 diabetes mellitus.
Keywords: blindness; complications; evidence-based medicine; myocardial infarction; type 2 diabetes mellitus.
© 2016 American Heart Association, Inc.
Conflict of interest statement
Disclosures: None.
Figures
References
-
- International Diabetes Federation. International Diabetes Federation diabetes atlas. 2014;2015
-
- The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The diabetes control and complications trial research group. New Engl J Med. 1993;329:977–986. - PubMed
-
- Pogach L, Aron DC. Sudden acceleration of diabetes quality measures. JAMA. 2011;305:709–710. - PubMed
-
- Garber AJ, Abrahamson MJ, Barzilay JI, Blonde L, Bloomgarden ZT, Bush MA, Dagogo-Jack S, Davidson MB, Einhorn D, Garvey WT, Grunberger G, Handelsman Y, Hirsch IB, Jellinger PS, McGill JB, Mechanick JI, Rosenblit PD, Umpierrez G, Davidson MH. Aace comprehensive diabetes management algorithm 2013. Endocr Pract. 2013;19:327–336. - PubMed
-
- Standards of medical care in diabetes–2007. Diabetes care. 2007;30(Suppl 1):S4–S41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
