

Compressed sensing real-time cine cardiovascular magnetic resonance: accurate assessment of left ventricular function in a single-breath-hold
- PMID: 27553656
- PMCID: PMC4995641
- DOI: 10.1186/s12968-016-0271-0
Compressed sensing real-time cine cardiovascular magnetic resonance: accurate assessment of left ventricular function in a single-breath-hold
Abstract
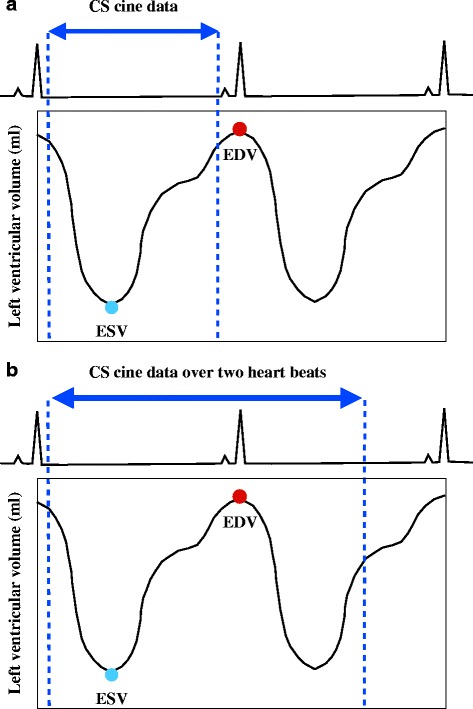
Background: Cardiovascular cine magnetic resonance (CMR) accelerated by compressed sensing (CS) is used to assess left ventricular (LV) function. However, it is difficult for prospective CS cine CMR to capture the complete end-diastolic phase, which can lead to underestimation of the end-diastolic volume (EDV), stroke volume (SV), and ejection fraction (EF), compared to retrospective standard cine CMR. This prospective study aimed to evaluate the diagnostic quality and accuracy of single-breath-hold full cardiac cycle CS cine CMR, acquired over two heart beats, to quantify LV volume in comparison to multi-breath-hold standard cine CMR.
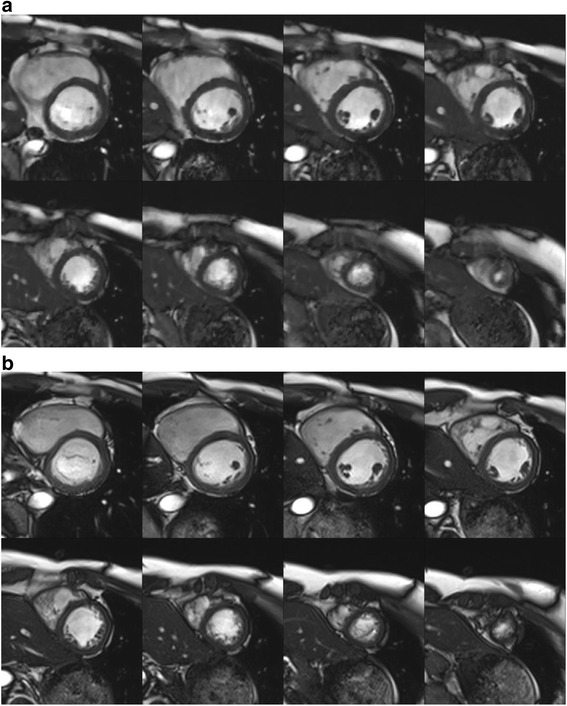
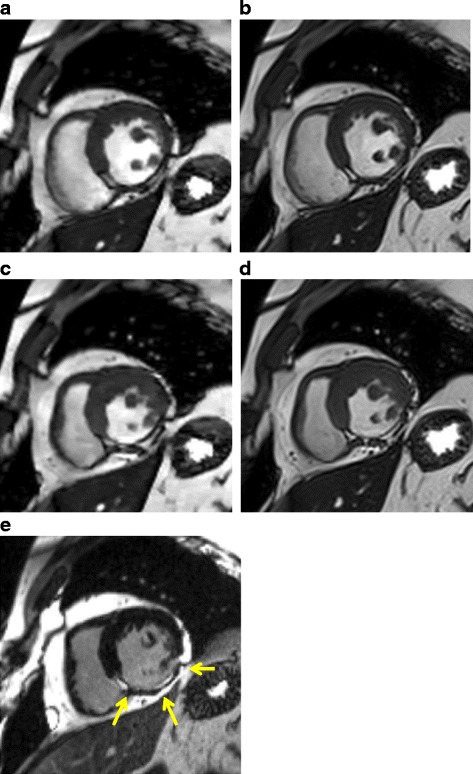
Methods: Eighty-one participants underwent standard segmented breath-hold cine and CS real-time cine CMR examinations to obtain a stack of eight contiguous short-axis images with same high spatial (1.7 × 1.7 mm(2)) and temporal resolution (41 ms). Two radiologists independently performed qualitative analysis of image quality (score, 1 [i.e., "nondiagnostic"] to 5 [i.e., "excellent"]) and quantitative analysis of the LV volume measurements.
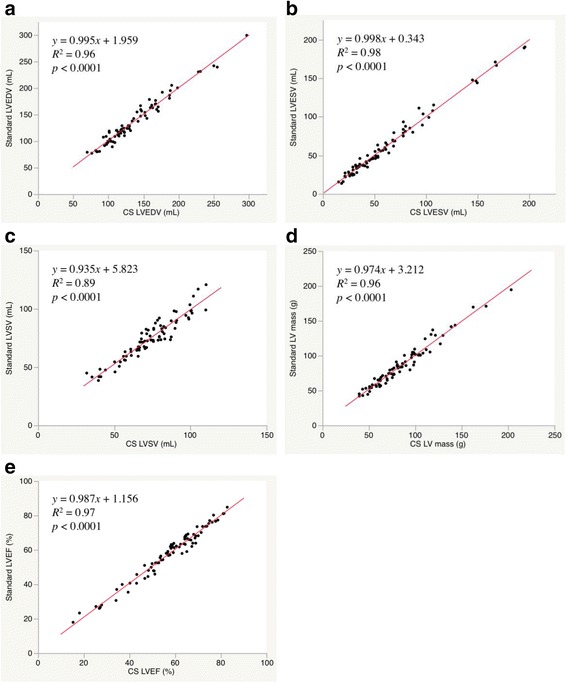
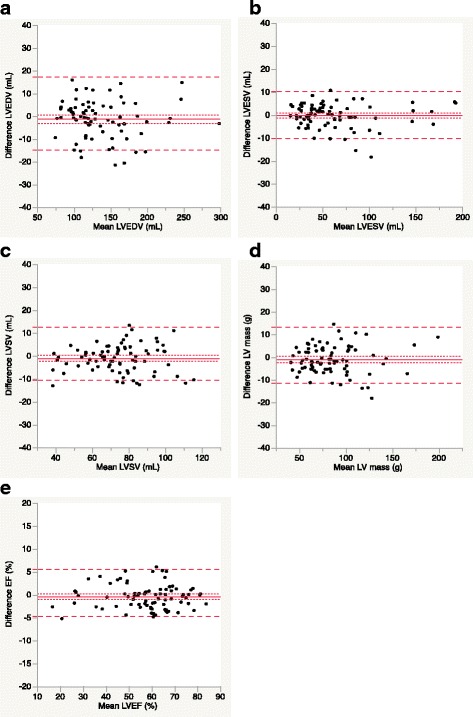
Results: The total examination time was 113 ± 7 s for standard cine CMR and 24 ± 4 s for CS cine CMR (p < 0.0001). The CS cine image quality was slightly lower than standard cine (4.8 ± 0.5 for standard vs. 4.4 ± 0.5 for CS; p < 0.0001). However, all image quality scores for CS cine were above 4 (i.e., good). No significant differences existed between standard and CS cine MR for all quantitative LV measurements. The mean differences with 95 % confidence interval (CI), based on Bland-Altman analysis, were 1.3 mL (95 % CI, -14.6 - 17.2) for LV end-diastolic volume, 0.2 mL (95 % CI, -9.8 to10.3) for LV end-systolic volume, 1.1 mL (95 % CI, -10.5 to 12.7) for LV stroke volume, 1.0 g (95 % CI, -11.2 to 13.3) for LV mass, and 0.4 % (95 % CI, -4.8 - 5.6) for LV ejection fraction. The interobserver and intraobserver variability for CS cine MR ranged from -4.8 - 1.6 % and from -7.3 - 9.3 %, respectively, with slopes of the regressions ranging 0.88-1.0 and 0.86-1.03, respectively.
Conclusions: Single-breath-hold full cardiac cycle CS real-time cine CMR could evaluate LV volume with excellent accuracy. It may replace multi-breath-hold standard cine CMR.
Keywords: Cardiac function; Cardiovascular magnetic resonance; Compressed sensing; Left ventricular ejection fraction; Real-time imaging.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
