

Personalized absolute benefit of statin treatment for primary or secondary prevention of vascular disease in individual elderly patients
- PMID: 27554244
- PMCID: PMC5226996
- DOI: 10.1007/s00392-016-1023-8
Personalized absolute benefit of statin treatment for primary or secondary prevention of vascular disease in individual elderly patients
Abstract
Objective: To estimate the absolute treatment effect of statin therapy on major adverse cardiovascular events (MACE; myocardial infarction, stroke and vascular death) for the individual patient aged ≥70 years.
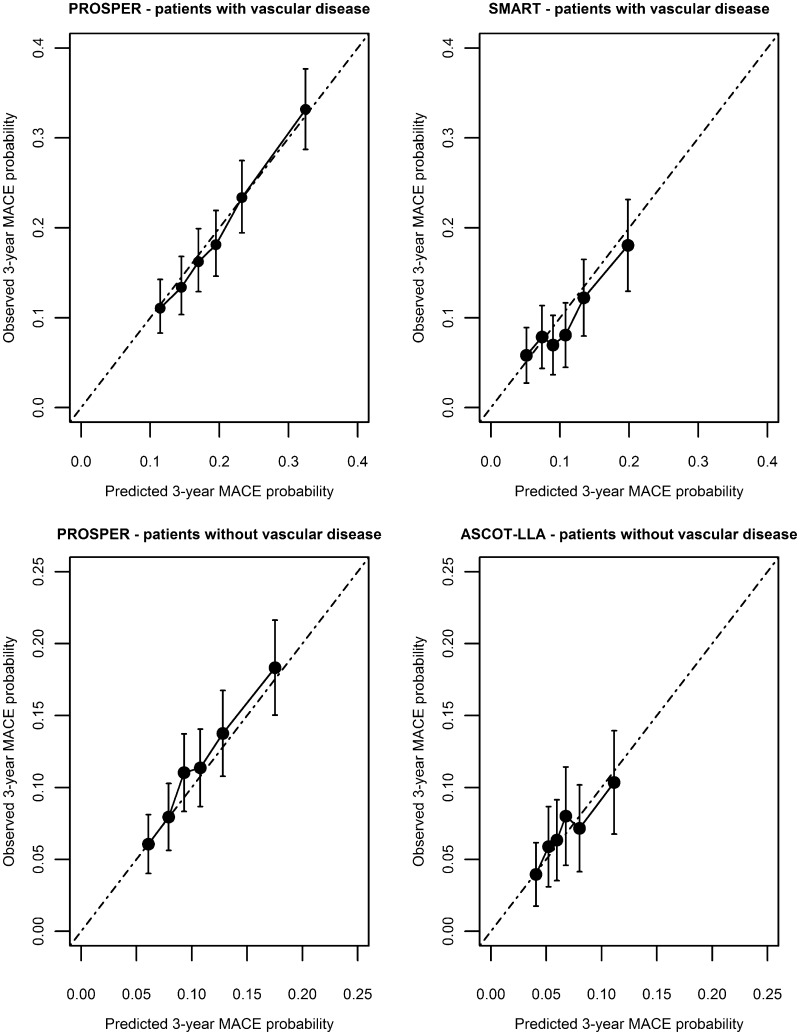
Methods: Prediction models for MACE were derived in patients aged ≥70 years with (n = 2550) and without (n = 3253) vascular disease from the "PROspective Study of Pravastatin in Elderly at Risk" (PROSPER) trial and validated in the "Secondary Manifestations of ARTerial disease" (SMART) cohort study (n = 1442) and the "Anglo-Scandinavian Cardiac Outcomes Trial-Lipid Lowering Arm" (ASCOT-LLA) trial (n = 1893), respectively, using competing risk analysis. Prespecified predictors were various clinical characteristics including statin treatment. Individual absolute risk reductions (ARRs) for MACE in 5 and 10 years were estimated by subtracting on-treatment from off-treatment risk.
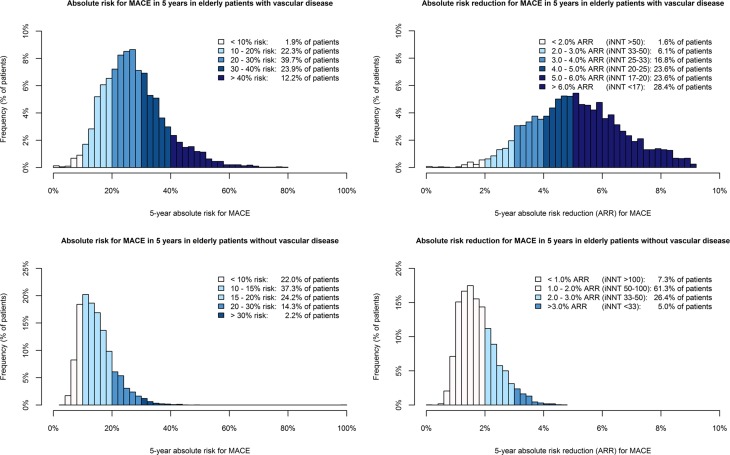
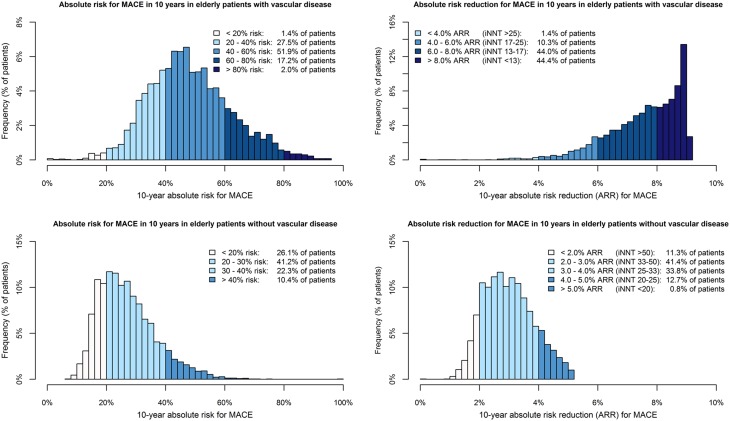
Results: Individual ARRs were higher in elderly patients with vascular disease [5-year ARRs: median 5.1 %, interquartile range (IQR) 4.0-6.2 %, 10-year ARRs: median 7.8 %, IQR 6.8-8.6 %] than in patients without vascular disease (5-year ARRs: median 1.7 %, IQR 1.3-2.1 %, 10-year ARRs: 2.9 %, IQR 2.3-3.6 %). Ninety-eight percent of patients with vascular disease had a 5-year ARR ≥2.0 %, compared to 31 % of patients without vascular disease.
Conclusions: With a multivariable prediction model the absolute treatment effect of a statin on MACE for individual elderly patients with and without vascular disease can be quantified. Because of high ARRs, treating all patients is more beneficial than prediction-based treatment for secondary prevention of MACE. For primary prevention of MACE, the prediction model can be used to identify those patients who benefit meaningfully from statin therapy.
Keywords: Absolute treatment effect; Elderly; Statin; Vascular disease.
Conflict of interest statement
JWJ/his department has received research grants from and/or was speaker (with or without lecture fees) on a.o. (CME accredited) meetings sponsored by Amgen, Astellas, Anthera, Astra-Zeneca, Bayer, Biotronik, Boston Scientific, Daiichi Sankyo, Lilly, Genzyme, Medtronic, Merck-Schering-Plough, Pfizer, Orbus Neich, Novartis, Roche, Servier, Sanofi Aventis, The Medicine Company, the Netherlands Heart Foundation, CardioVascular Research the Netherlands (CVON), the Interuniversity Cardiology Institute of the Netherlands and the European Community Framework KP7 Programme. AG received a travel grant from Pfizer inc. NS reports personal fees from Amgen, personal fees from Astrazeneca, personal fees from Merck, during the conduct of the study. MCS-S, FLJV, YvdG, NRP, PWM, PKM and ST have nothing to disclose. Ethical standards All studies have been approved by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All persons gave their informed consent prior to their inclusion in the study.
Figures
References
-
- Jaguszewski M, Ghadri JR, Diekmann J, Bataiosu RD, Hellermann JP, Sarcon A, Siddique A, Baumann L, Stahli BE, Luscher TF, Maier W, Templin C. Acute coronary syndromes in octogenarians referred for invasive evaluation: treatment profile and outcomes. Clin Res Cardiol. 2015;104:51–58. doi: 10.1007/s00392-014-0756-5. - DOI - PubMed
-
- Shepherd J, Blauw GJ, Murphy MB, Bollen EL, Buckley BM, Cobbe SM, Ford I, Gaw A, Hyland M, Jukema JW, Kamper AM, Macfarlane PW, Meinders AE, Norrie J, Packard CJ, Perry IJ, Stott DJ, Sweeney BJ, Twomey C, Westendorp RG. Pravastatin in elderly individuals at risk of vascular disease (PROSPER): a randomised controlled trial. Lancet. 2002;360:1623–1630. doi: 10.1016/S0140-6736(02)11600-X. - DOI - PubMed
-
- Kutner JS, Blatchford PJ, Taylor DH, Jr, Ritchie CS, Bull JH, Fairclough DL, Hanson LC, LeBlanc TW, Samsa GP, Wolf S, Aziz NM, Currow DC, Ferrell B, Wagner-Johnston N, Zafar SY, Cleary JF, Dev S, Goode PS, Kamal AH, Kassner C, Kvale EA, McCallum JG, Ogunseitan AB, Pantilat SZ, Portenoy RK, Prince-Paul M, Sloan JA, Swetz KM, Von Gunten CF, Abernethy AP. Safety and benefit of discontinuing statin therapy in the setting of advanced, life-limiting illness: a randomized clinical trial. JAMA Intern Med. 2015;175:691–700. doi: 10.1001/jamainternmed.2015.0289. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
