

Investigating the nature of co-occurring depression and anxiety: Comparing diagnostic and dimensional research approaches
- PMID: 27554605
- PMCID: PMC5308464
- DOI: 10.1016/j.jad.2016.08.006
Investigating the nature of co-occurring depression and anxiety: Comparing diagnostic and dimensional research approaches
Abstract
Background: Although approximately half of adults diagnosed with a depressive or anxiety disorder exhibit their simultaneous co-occurrence, traditional research has centered on single-target diagnoses, overlooking comorbidities within samples. In this article, we review and extend the literature that directly investigates co-occurring depression and anxiety, with the goal of shifting the focus from co-occurring diagnoses to symptom dimensions.
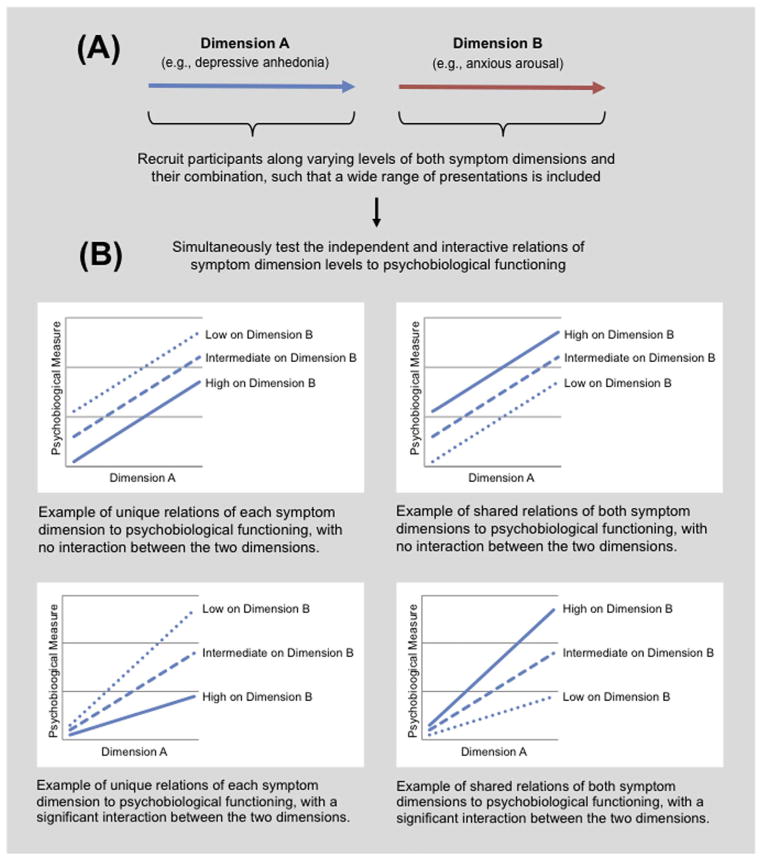
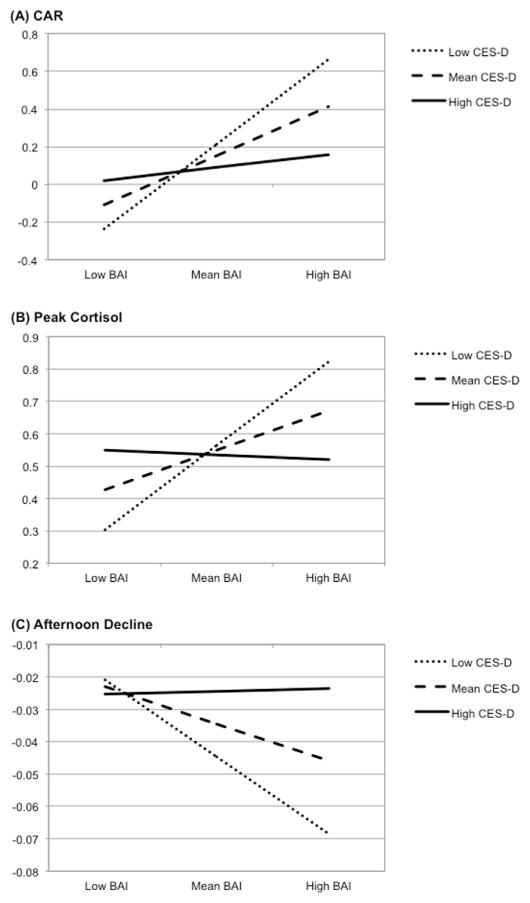
Methods: First, we review studies that have directly compared psychobiological features (neural, neuroendocrine, autonomic) across depression, anxiety, and their co-occurrence, defined either categorically or dimensionally. Second, we analyze adults' diurnal cortisol secretion to examine the independent and interactive relations of continuously-assessed depressive and anxiety symptoms to neuroendocrine function.
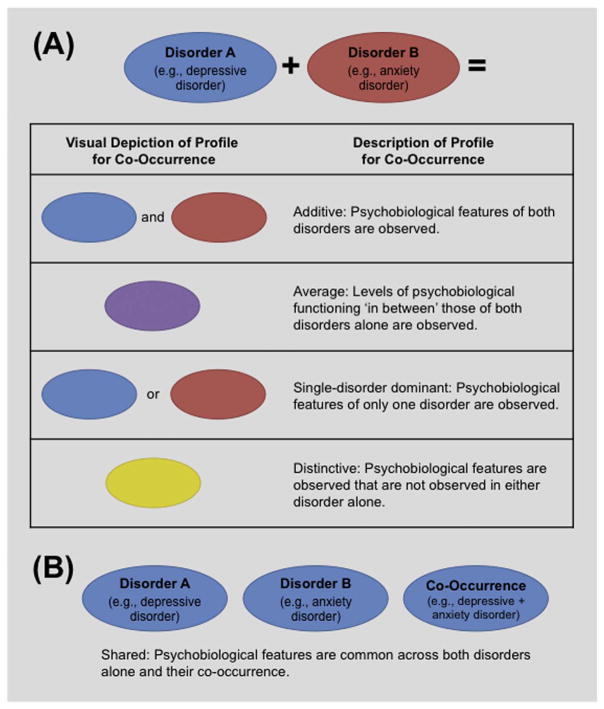
Results: Previous findings on the psychobiology of diagnostic co-occurrence are mixed. While nascent, evidence from dimensionally focused studies suggests that co-occurring levels of depressive and anxiety symptoms can interact with one another, as reflected in a distinct psychobiological profile for individuals with high levels of both symptom dimensions. Results of our analyses support this formulation: we found that depressive and anxiety symptom dimensions interacted consistently in their relation to the measures of diurnal cortisol.
Limitations: The illustrative sample was relatively small and included only women; future research should examine generalizability of these findings.
Conclusions: A dimensional approach to investigating the psychobiology of co-occurring depression and anxiety affords both conceptual and practical advantages. Simultaneously assessing depressive and anxiety symptom dimensions can efficiently capture their unique, shared, and interactive features, thereby identifying targets for intervention across a wide range of symptom presentations.
Keywords: Anxiety; Comorbidity; Cortisol; Depression; Symptom dimension.
Published by Elsevier B.V.
Figures
References
-
- Andrews G, Hobbs MJ, Borkovec TD, Beesdo K, Craske MG, Heimberg RG, Stanley MA. Generalized worry disorder: a review of DSM-IV generalized anxiety disorder and options for DSM-V. Depress. Anxiety. 2010;27:134–147. - PubMed
-
- van Balkom AJLM, van Boeijen CA, Boeke AJP, van Oppen P, Kempe PT, van Dyck R. Comorbid depression, but not comorbid anxiety disorders, predicts poor outcome in anxiety disorders. Depress Anxiety. 2008;25:408–415. - PubMed
-
- Ballenger JC, Davidson JR, Lecrubier Y, Nutt DJ, Borkovec TD, Rickels K, Wittchen HU. Consensus statement on generalized anxiety disorder from the International Consensus Group on Depression and Anxiety. J Clin Psychiatry. 2001;62:53–58. - PubMed
-
- Barlow DH. Anxiety and Its Disorders: The Nature and Treatment of Anxiety and Panic. Guilford Press; New York: 2002.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
