

Intermediate and Long-term Outcomes of Survivors of Acute Kidney Injury Episodes: A Large Population-Based Cohort Study
- PMID: 27555107
- PMCID: PMC5176133
- DOI: 10.1053/j.ajkd.2016.05.018
Intermediate and Long-term Outcomes of Survivors of Acute Kidney Injury Episodes: A Large Population-Based Cohort Study
Abstract
Background: The long-term prognosis after acute kidney injury (AKI) is variable. It is unclear how the prognosis of AKI and its relationship to prognostic factors (baseline kidney function, AKI severity, prior AKI episodes, and recovery of kidney function) change as follow-up progresses.
Study design: Observational cohort study.
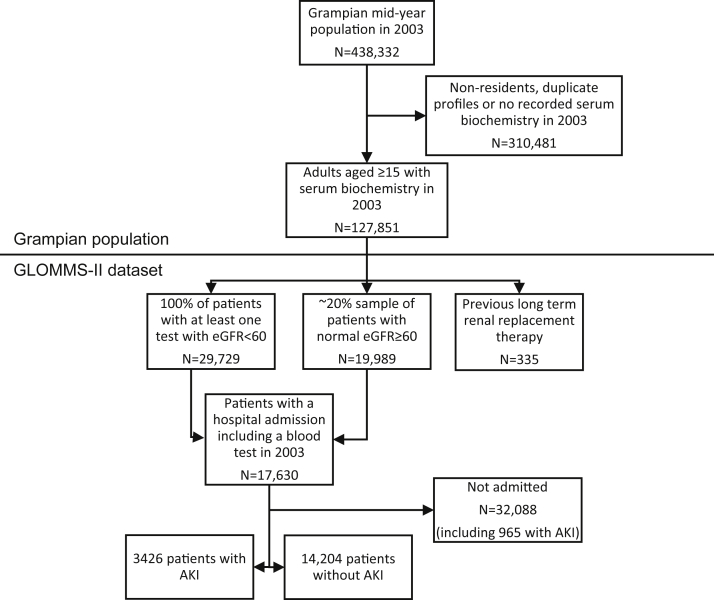
Setting & participants: The Grampian Laboratory Outcomes Morbidity and Mortality Study II (GLOMMS-II) is a large regional population cohort with complete serial biochemistry and outcome data capture through data linkage. From GLOMMS-II, we followed up 17,630 patients hospitalized in 2003 through to 2013.
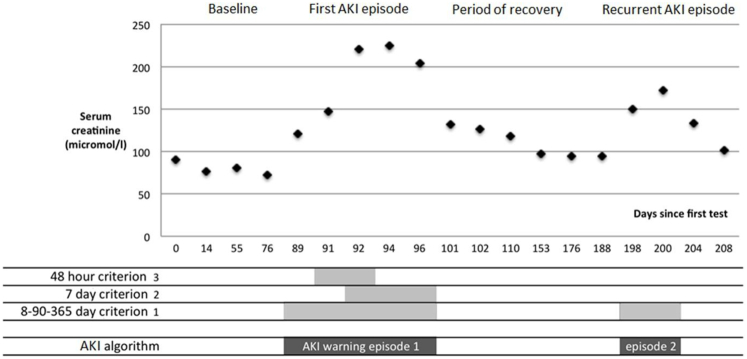
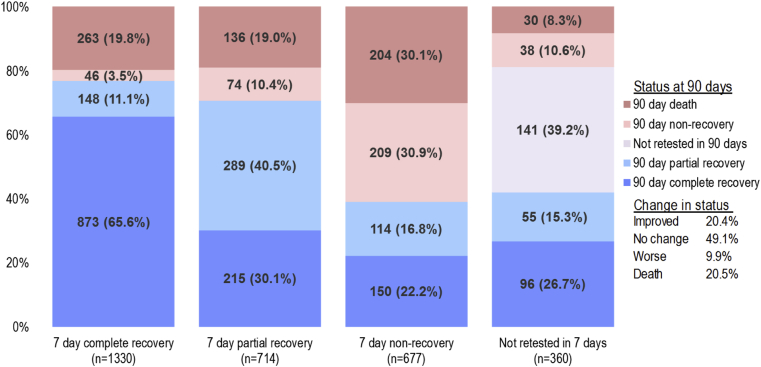
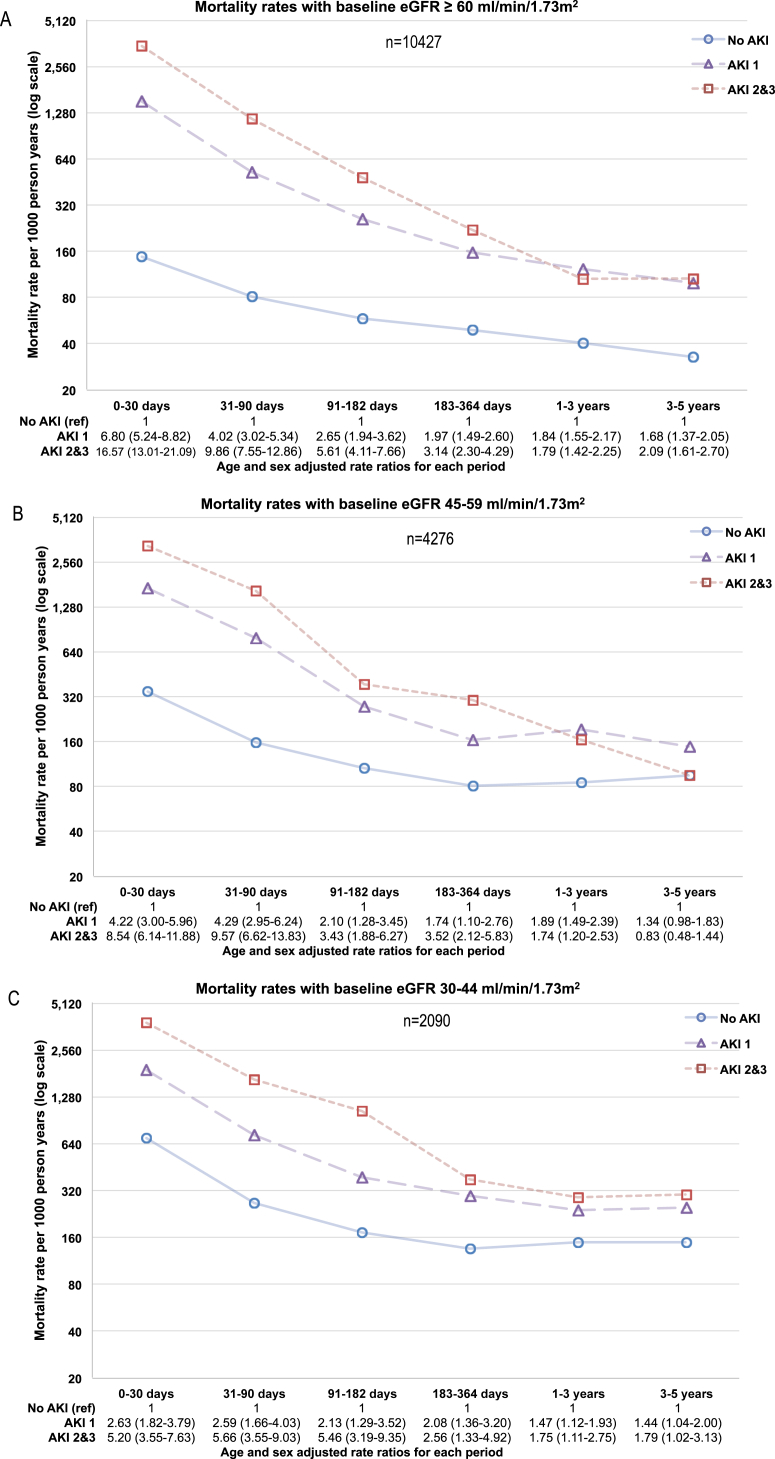
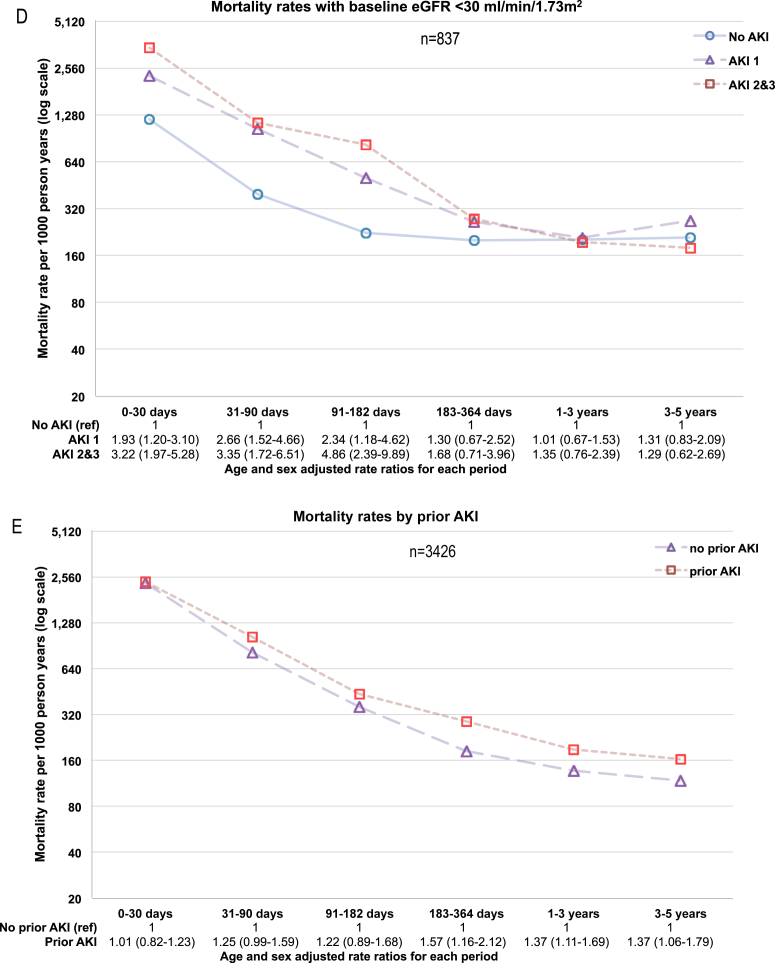
Predictors: AKI identified using KDIGO (Kidney Disease: Improving Global Outcomes) serum creatinine criteria, characterized by baseline kidney function (estimated glomerular filtration rate [eGFR] ≥ 60, 45-59, 30-44, and <30mL/min/1.73m2), AKI severity (KDIGO stage), 90-day recovery of kidney function, and prior AKI episodes.
Outcomes: Intermediate- (30-364 days) and long-term (1-10 years) mortality and long-term renal replacement therapy.
Measurements: Poisson regression in time discrete intervals. Multivariable Cox regression for those at risk in the intermediate and long term, adjusted for age, sex, baseline comorbid conditions, and acute admission circumstances.
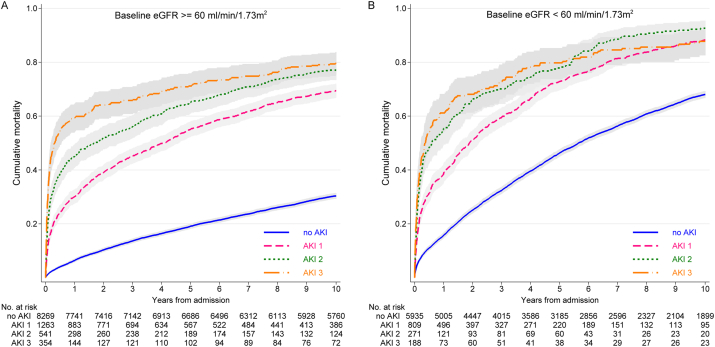
Results: Of 17,630 patients followed up for a median of 9.0 years, 9,251 died. Estimated incidences of hospital AKI were 8.4% and 17.6% for baseline eGFRs≥60 and <60mL/min/1.73m2, respectively. Intermediate-term (30-364 days) adjusted mortality HRs for AKI versus no AKI were 2.48 (95% CI, 2.15-2.88), 2.50 (95% CI, 2.04-3.06), 1.90 (95% CI, 1.51-2.39), and 1.63 (95% CI, 1.20-2.22) for eGFRs≥60, 45 to 59, 30 to 44, and <30mL/min/1.73m2, respectively. Among 1-year survivors, long-term HRs were attenuated: 1.44 (95% CI, 1.31-1.58), 1.25 (95% CI, 1.09-1.43), 1.21 (95% CI, 1.03-1.42), and 1.08 (95% CI, 0.85-1.36), respectively. The excess long-term hazards in AKI were lower for lower baseline eGFRs (P for interaction = 0.01).
Limitations: Nonprotocolized observational data. No adjustment for albuminuria.
Conclusions: The prognostic importance of a discrete AKI episode lessens over time. Baseline kidney function is of greater long-term importance.
Keywords: AKI recovery; Acute kidney injury (AKI); acute on chronic kidney disease; baseline kidney function; chronic kidney disease (CKD); epidemiology; mortality; outcomes; prognosis; survival.
Copyright © 2016 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Long-term Outcomes of Acute Kidney Injury: The Power and Pitfalls of Observational/Population-Based Studies.Am J Kidney Dis. 2017 Jan;69(1):3-4. doi: 10.1053/j.ajkd.2016.10.004. Am J Kidney Dis. 2017. PMID: 28007191 No abstract available.
-
Long-term Outcomes of Survivors of Acute Kidney Injury Stage 3.Am J Kidney Dis. 2017 May;69(5):705. doi: 10.1053/j.ajkd.2016.10.042. Epub 2017 Feb 21. Am J Kidney Dis. 2017. PMID: 28233654 No abstract available.
-
In Reply to 'Long-term Outcomes of Survivors of Acute Kidney Injury Stage 3'.Am J Kidney Dis. 2017 May;69(5):705-706. doi: 10.1053/j.ajkd.2016.12.014. Epub 2017 Feb 23. Am J Kidney Dis. 2017. PMID: 28237312 No abstract available.
References
-
- Chertow G.M., Burdick E., Honour M., Bonventre J.V., Bates D.W. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol. 2005;16(11):3365–3370. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
