

Inflammatory and Comorbid Features of Patients with Severe Asthma and Frequent Exacerbations
- PMID: 27556234
- PMCID: PMC5328178
- DOI: 10.1164/rccm.201602-0419OC
Inflammatory and Comorbid Features of Patients with Severe Asthma and Frequent Exacerbations
Erratum in
-
Erratum: Inflammatory and Comorbid Features of Patients with Severe Asthma and Frequent Exacerbations.Am J Respir Crit Care Med. 2018 Apr 1;197(7):971. doi: 10.1164/rccm.1977erratum2. Am J Respir Crit Care Med. 2018. PMID: 30907097 Free PMC article. No abstract available.
Abstract
Rationale: Reducing asthma exacerbation frequency is an important criterion for approval of asthma therapies, but the clinical features of exacerbation-prone asthma (EPA) remain incompletely defined.
Objectives: To describe the clinical, physiologic, inflammatory, and comorbidity factors associated with EPA.
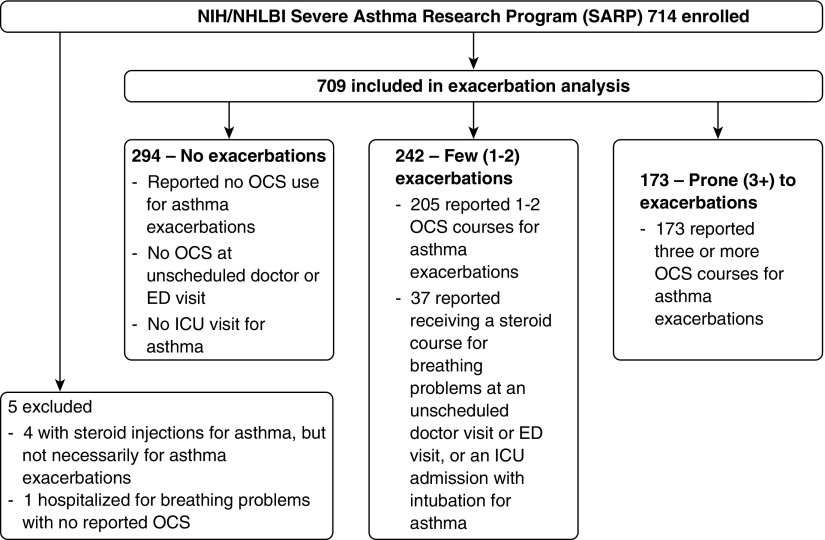
Methods: Baseline data from the NHLBI Severe Asthma Research Program (SARP)-3 were analyzed. An exacerbation was defined as a burst of systemic corticosteroids lasting 3 days or more. Patients were classified by their number of exacerbations in the past year: none, few (one to two), or exacerbation prone (≥3). Replication of a multivariable model was performed with data from the SARP-1 + 2 cohort.
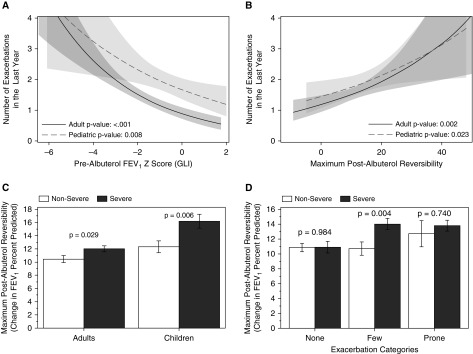
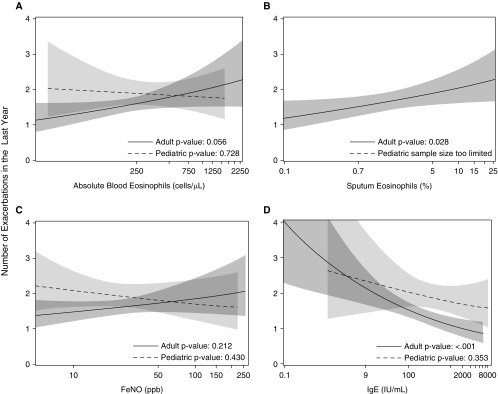
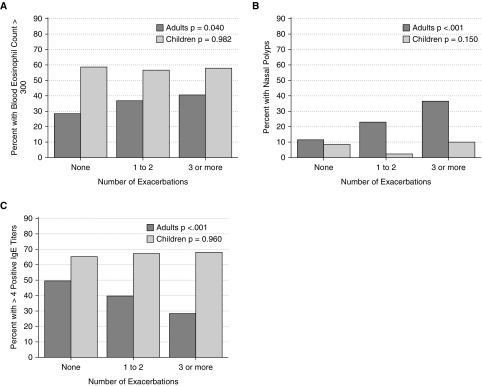
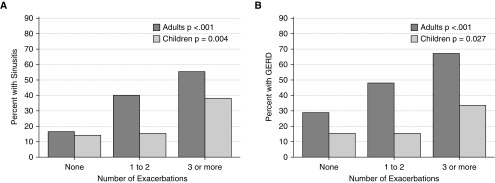
Measurements and main results: Of 709 subjects in the SARP-3 cohort, 294 (41%) had no exacerbations and 173 (24%) were exacerbation prone in the prior year. Several factors normally associated with severity (asthma duration, age, sex, race, and socioeconomic status) did not associate with exacerbation frequency in SARP-3; bronchodilator responsiveness also discriminated exacerbation proneness from asthma severity. In the SARP-3 multivariable model, blood eosinophils, body mass index, and bronchodilator responsiveness were positively associated with exacerbation frequency (rate ratios [95% confidence interval], 1.6 [1.2-2.1] for every log unit of eosinophils, 1.3 [1.1-1.4] for every 10 body mass index units, and 1.2 [1.1-1.4] for every 10% increase in bronchodilatory responsiveness). Chronic sinusitis and gastroesophageal reflux were also associated with exacerbation frequency (1.7 [1.4-2.1] and 1.6 [1.3-2.0]), even after adjustment for multiple factors. These effects were replicated in the SARP-1 + 2 multivariable model.
Conclusions: EPA may be a distinct susceptibility phenotype with implications for the targeting of exacerbation prevention strategies. Clinical trial registered with www.clinicaltrials.gov (NCT 01760915).
Trial registration: ClinicalTrials.gov NCT01760915.
Keywords: bronchodilator reversibility; eosinophils; exacerbation-prone asthma; gastroesophageal reflux; sinusitis.
Figures
Comment in
-
Exacerbation-Prone Asthma: A Separate Bioclinical Phenotype?Am J Respir Crit Care Med. 2017 Feb 1;195(3):275-277. doi: 10.1164/rccm.201609-1819ED. Am J Respir Crit Care Med. 2017. PMID: 28145763 No abstract available.
References
-
- Tattersfield AE, Postma DS, Barnes PJ, Svensson K, Bauer CA, O’Byrne PM, Löfdahl CG, Pauwels RA, Ullman A The FACET International Study Group. Exacerbations of asthma: a descriptive study of 425 severe exacerbations. Am J Respir Crit Care Med. 1999;160:594–599. - PubMed
-
- Dolan CM, Fraher KE, Bleecker ER, Borish L, Chipps B, Hayden ML, Weiss S, Zheng B, Johnson C, Wenzel S TENOR Study Group. Design and baseline characteristics of the epidemiology and natural history of asthma: Outcomes and Treatment Regimens (TENOR) study: a large cohort of patients with severe or difficult-to-treat asthma. Ann Allergy Asthma Immunol. 2004;92:32–39. - PubMed
-
- Moore WC, Bleecker ER, Curran-Everett D, Erzurum SC, Ameredes BT, Bacharier L, Calhoun WJ, Castro M, Chung KF, Clark MP, et al. National Heart, Lung, Blood Institute’s Severe Asthma Research Program. Characterization of the severe asthma phenotype by the National Heart, Lung, and Blood Institute’s Severe Asthma Research Program. J Allergy Clin Immunol. 2007;119:405–413. - PMC - PubMed
-
- Griswold SK, Nordstrom CR, Clark S, Gaeta TJ, Price ML, Camargo CA., Jr Asthma exacerbations in North American adults: who are the “frequent fliers” in the emergency department? Chest. 2005;127:1579–1586. - PubMed
-
- ten Brinke A, Sterk PJ, Masclee AA, Spinhoven P, Schmidt JT, Zwinderman AH, Rabe KF, Bel EH. Risk factors of frequent exacerbations in difficult-to-treat asthma. Eur Respir J. 2005;26:812–818. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U10 HL109257/HL/NHLBI NIH HHS/United States
- UL1 TR000427/TR/NCATS NIH HHS/United States
- K23 AI106945/AI/NIAID NIH HHS/United States
- T32 AI007635/AI/NIAID NIH HHS/United States
- K12 HL119997/HL/NHLBI NIH HHS/United States
- R01 HL122531/HL/NHLBI NIH HHS/United States
- U10 HL109164/HL/NHLBI NIH HHS/United States
- U10 HL109086/HL/NHLBI NIH HHS/United States
- U10 HL109172/HL/NHLBI NIH HHS/United States
- U10 HL064313/HL/NHLBI NIH HHS/United States
- K23 HL116657/HL/NHLBI NIH HHS/United States
- R01 HL115118/HL/NHLBI NIH HHS/United States
- U10 HL109250/HL/NHLBI NIH HHS/United States
- UL1 RR025011/RR/NCRR NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- UL1 TR001420/TR/NCATS NIH HHS/United States
- U10 HL109168/HL/NHLBI NIH HHS/United States
- UL1 TR001102/TR/NCATS NIH HHS/United States
- U10 HL109152/HL/NHLBI NIH HHS/United States
- U10 HL109146/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
