

Non-falciparum malaria in Dakar: a confirmed case of Plasmodium ovale wallikeri infection
- PMID: 27557982
- PMCID: PMC4997729
- DOI: 10.1186/s12936-016-1485-1
Non-falciparum malaria in Dakar: a confirmed case of Plasmodium ovale wallikeri infection
Abstract
Background: Plasmodium ovale is rarely described in Senegal. A case of clinical malaria due to P. ovale wallikeri in West Central of Senegal is reported.
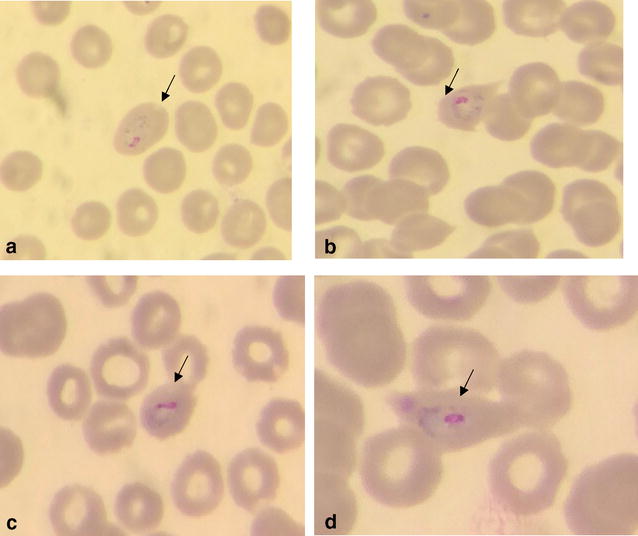
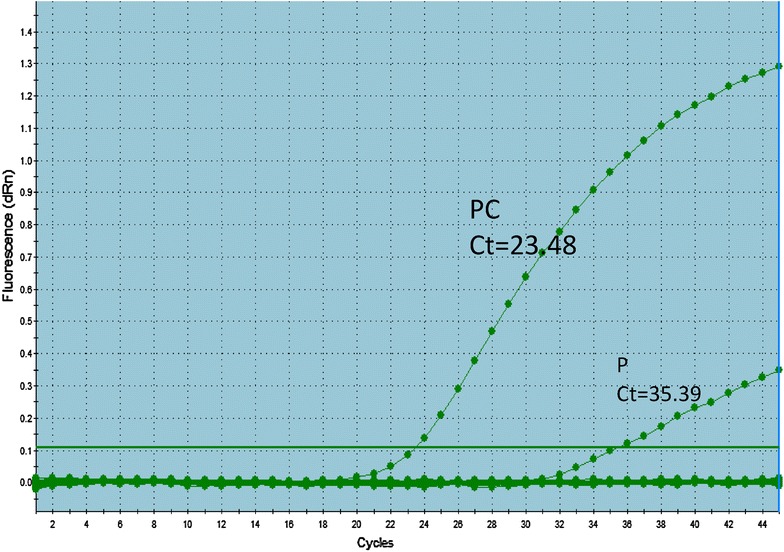
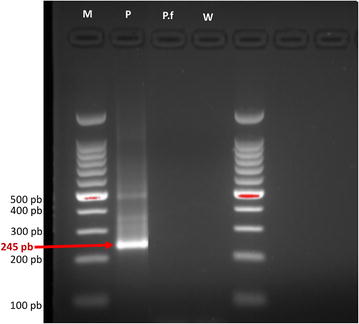
Case: A 34-year-old male baker in Dakar, with no significant previous medical history, was admitted to a health clinic with fever and vomiting. Fever had been lasting for 4 days with peaks every 48 h. As monospecific Plasmodium falciparum HRP-2 RDT was negative, he was treated with antibiotics. However, owing to persisting symptoms, he was referred to the emergency unit of the Youssou Mbargane Diop Hospital, Dakar, Senegal. Clinical examination found impaired general condition. All other physical examinations were normal. Laboratory tests showed anaemia (haemoglobin 11.4 g/dl), severe thrombocytopaenia (platelets 30 × 10(9)/mm(3)), leukopenia (3650/mm(3)), lymphocytopenia (650/mm(3)). Renal function was normal as indicated by creatininaemia and uraemia (11 mg/l and 0.25 g/l, respectively) and liver enzymes were slightly elevated (aspartate aminotransferase 77 UI/l and alanine aminotransferase 82 UI/l). Blood smear evaluations in Parasitology Laboratory of Aristide Le Dantec Hospital showed malaria parasites of the species P. ovale with a 0.08 % parasitaemia. Molecular confirmation was done by real time PCR targeting the 18S rRNA gene. The P. ovale infection was further analysed to species level targeting the potra gene and was identified as P. ovale wallikeri. According to the hospital's malaria treatment guidelines for severe malaria, treatment consisted of intravenous quinine at hour 0 (start of treatment) and 24 h after initial treatment, followed by artemether-lumefantrine 24 h later. A negative microscopy was noted on day 3 post-treatment and the patient reported no further symptoms.
Conclusion: Malaria due to non-falciparum species is probably underestimated in Senegal. RDTs specific to non-falciparum species and/or pan specific RDTs should be included as tools of diagnosis to fight against malaria in Senegal. In addition, a field-deployable molecular tool such as the loop-mediated isothermal amplification can be considered as an additional useful tool to detect low malaria parasite infections and for speciation. In addition, national malaria control policies should consider other non-falciparum species in treatment guidelines, including the provision of primaquine for the treatment of relapsing parasites.
Keywords: Dakar; Diagnostic; Fever; Malaria; Microscopy; Plasmodium ovale; Primaquine; RDT; Treatment.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
