

Ovarian cancer
- PMID: 27558151
- PMCID: PMC7290868
- DOI: 10.1038/nrdp.2016.61
Ovarian cancer
Abstract
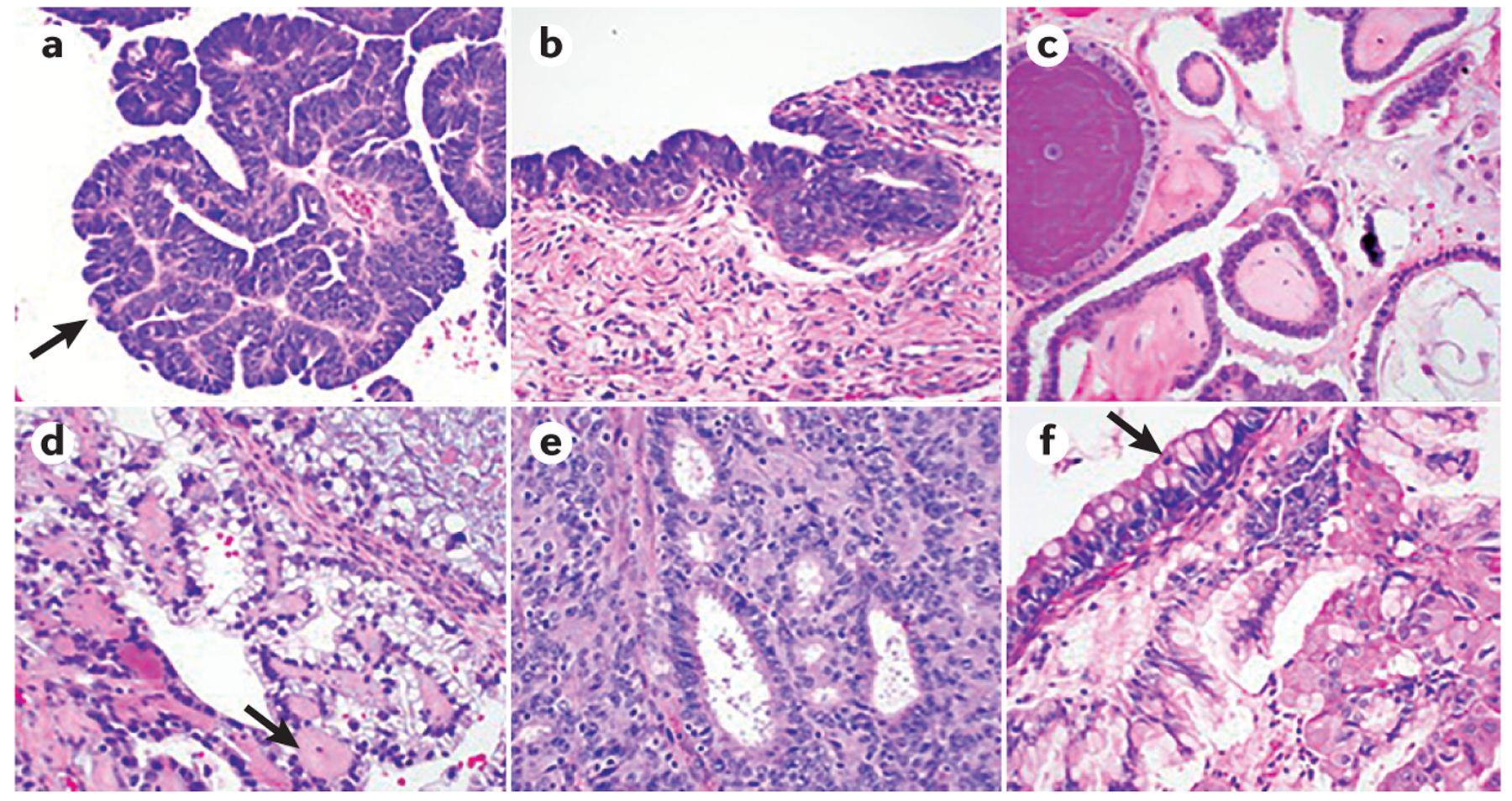
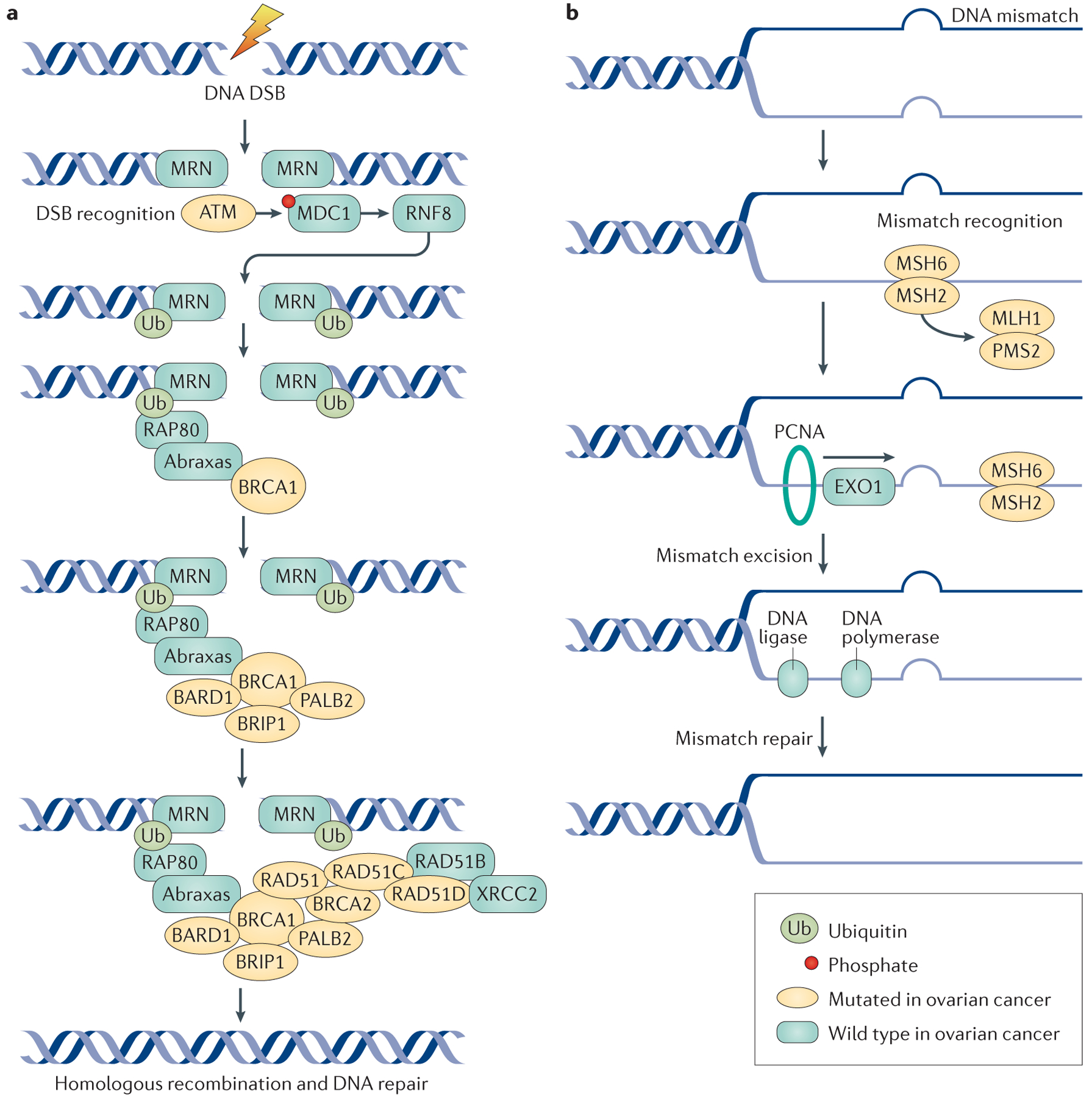
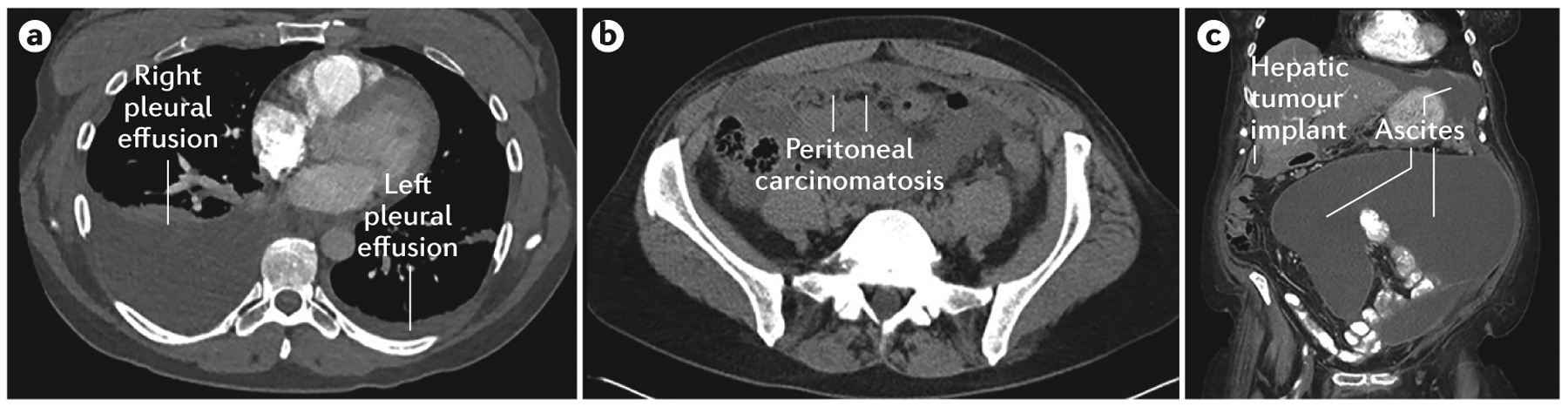
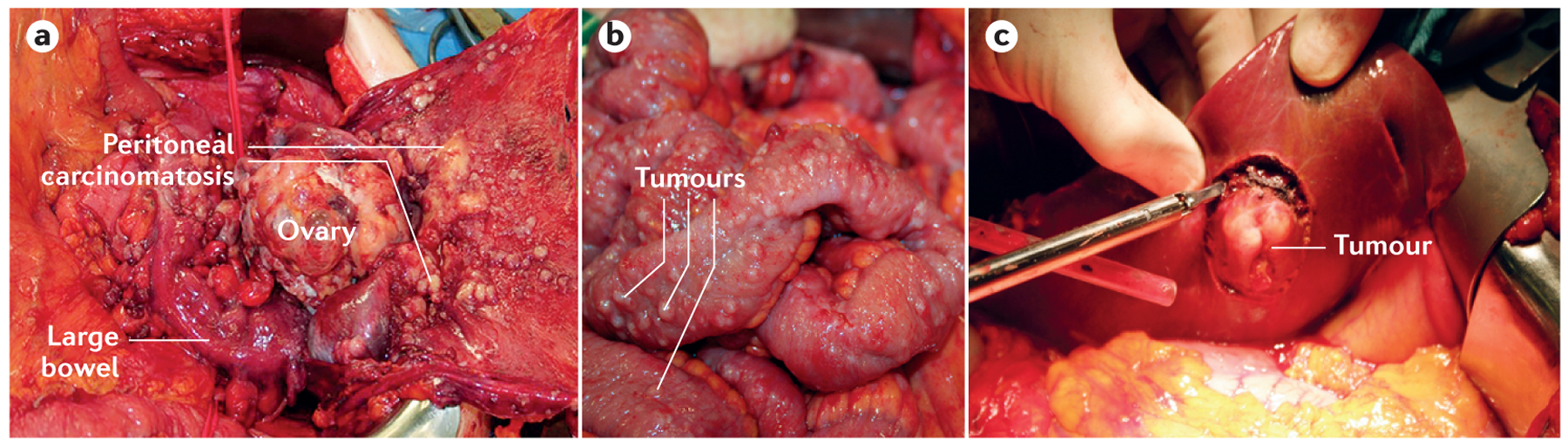
Ovarian cancer is not a single disease and can be subdivided into at least five different histological subtypes that have different identifiable risk factors, cells of origin, molecular compositions, clinical features and treatments. Ovarian cancer is a global problem, is typically diagnosed at a late stage and has no effective screening strategy. Standard treatments for newly diagnosed cancer consist of cytoreductive surgery and platinum-based chemotherapy. In recurrent cancer, chemotherapy, anti-angiogenic agents and poly(ADP-ribose) polymerase inhibitors are used, and immunological therapies are currently being tested. High-grade serous carcinoma (HGSC) is the most commonly diagnosed form of ovarian cancer and at diagnosis is typically very responsive to platinum-based chemotherapy. However, in addition to the other histologies, HGSCs frequently relapse and become increasingly resistant to chemotherapy. Consequently, understanding the mechanisms underlying platinum resistance and finding ways to overcome them are active areas of study in ovarian cancer. Substantial progress has been made in identifying genes that are associated with a high risk of ovarian cancer (such as BRCA1 and BRCA2), as well as a precursor lesion of HGSC called serous tubal intraepithelial carcinoma, which holds promise for identifying individuals at high risk of developing the disease and for developing prevention strategies.
Conflict of interest statement
Competing interests
U.A.M. has served as a consultant for AstraZeneca, ImmunoGen, Pfizer, Genentech and Merck. All other authors declare no competing interests.
Figures
References
-
- Oswald AJ & Gourley C Low-grade epithelial ovarian cancer: a number of distinct clinical entities? Curr. Opin. Oncol 27, 412–419 (2015). - PubMed
-
- Groen RS, Gershenson DM & Fader AN Updates and emerging therapies for rare epithelial ovarian cancers: one size no longer fits all. Gynecol. Oncol 136, 373–383 (2015). - PubMed
-
- Mangili G et al. Unraveling the two entities of endometrioid ovarian cancer: a single center clinical experience. Gynecol. Oncol 126, 403–407 (2012). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
