

The impact of long-lasting microbial larvicides in reducing malaria transmission and clinical malaria incidence: study protocol for a cluster randomized controlled trial
- PMID: 27558161
- PMCID: PMC4997667
- DOI: 10.1186/s13063-016-1545-4
The impact of long-lasting microbial larvicides in reducing malaria transmission and clinical malaria incidence: study protocol for a cluster randomized controlled trial
Abstract
Background: The massive scale-up of insecticide-treated nets (ITNs) and indoor residual spraying (IRS) has led to a substantial increase in malaria vector insecticide resistance as well as in increased outdoor transmission, both of which hamper the effectiveness and efficiency of ITN and IRS. Long-lasting microbial larvicide can be a cost-effective new supplemental intervention tool for malaria control.
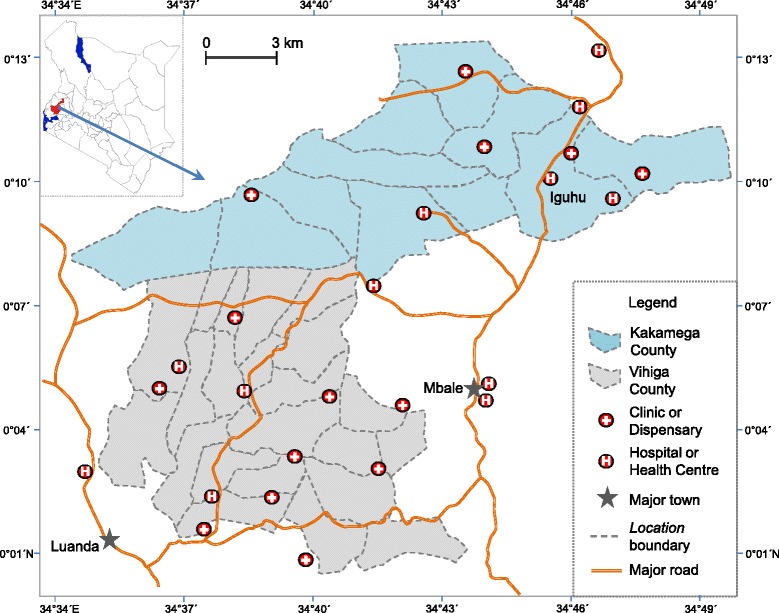
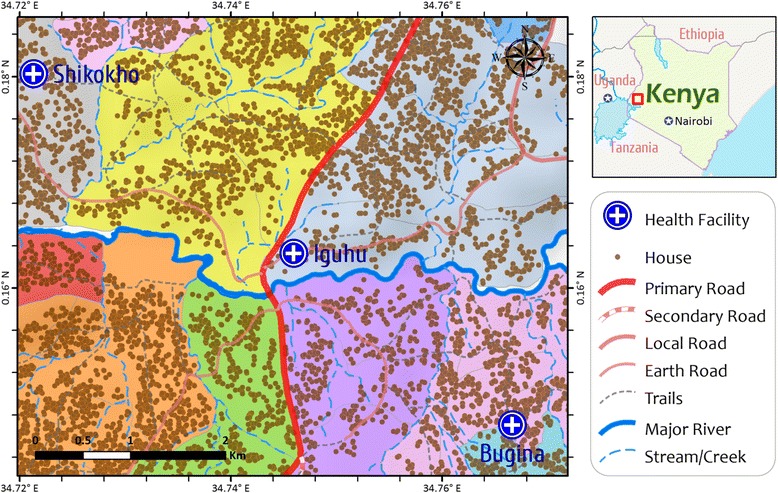
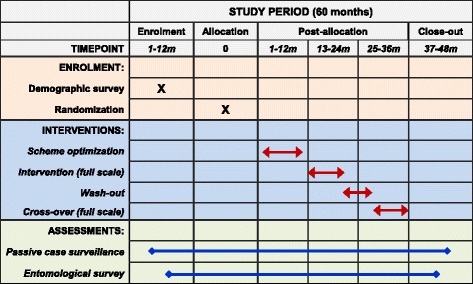
Methods/design: We will implement the long-lasting microbial larvicide intervention in 28 clusters in two counties in western Kenya. We will test FourStar controlled release larvicide (6 % by weight Bacillus thuringiensis israelensis and 1 % Bacillus sphaerius) by applying FourStar controlled release granule formulation, 90-day briquettes, and 180-day briquettes in different habitat types. The primary endpoint is clinical malaria incidence rate and the secondary endpoint is malaria vector abundance and transmission intensity. The intervention will be conducted as a two-step approach. First, we will conduct a four-cluster trial (two clusters per county, with one of the two clusters randomly assigned to the intervention arm) to optimize the larvicide application scheme. Second, we will conduct an open-label, cluster-randomized trial to evaluate the effectiveness and cost-effectiveness of the larvicide. Fourteen clusters in each county will be assigned to intervention (treatment) or no intervention (control) by a block randomization on the basis of clinical malaria incidence, vector density, and human population size per site. We will treat each treatment cluster with larvicide for three rounds at 4-month intervals, followed by no treatment for the following 8 months. Next, we will switch the control and treatment sites. The former control sites will receive three rounds of larvicide treatment at appropriate time intervals, and former treatment sites will receive no larvicide. We will monitor indoor and outdoor vector abundance using CO2-baited CDC light traps equipped with collection bottle rotators. Clinical malaria data will be aggregated from government-run malaria treatment centers.
Discussion: Since current first-line vector intervention methods do not target outdoor transmission and will select for higher insecticide resistance, new methods beyond bed nets and IRS should be considered. Long-lasting microbial larviciding represents a promising new tool that can target both indoor and outdoor transmission and alleviate the problem of pyrethroid resistance. It also has the potential to diminish costs by reducing larvicide reapplications. If successful, it could revolutionize malaria vector control in Africa, just as long-lasting bed nets have done.
Trial registration: U.S. National Institute of Health, study ID NCT02392832 . Registered on 3 February 2015.
Keywords: Clinical malaria; Cluster-randomized controlled trial; Cost-effectiveness; Long-lasting microbial larvicide; Malaria transmission intensity; Vector abundance.
Figures
References
-
- World Health Organization . World Malaria Report 2012. Geneva: WHO; 2012.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
