

Tibiopedal Access for Crossing of Infrainguinal Artery Occlusions: A Prospective Multicenter Observational Study
- PMID: 27558463
- PMCID: PMC5315197
- DOI: 10.1177/1526602816664768
Tibiopedal Access for Crossing of Infrainguinal Artery Occlusions: A Prospective Multicenter Observational Study
Abstract
Purpose: To report a prospective, multicenter, observational study (ClinicalTrials.gov identifier NCT01609621) of the safety and effectiveness of tibiopedal access and retrograde crossing in the treatment of infrainguinal chronic total occlusions (CTOs).
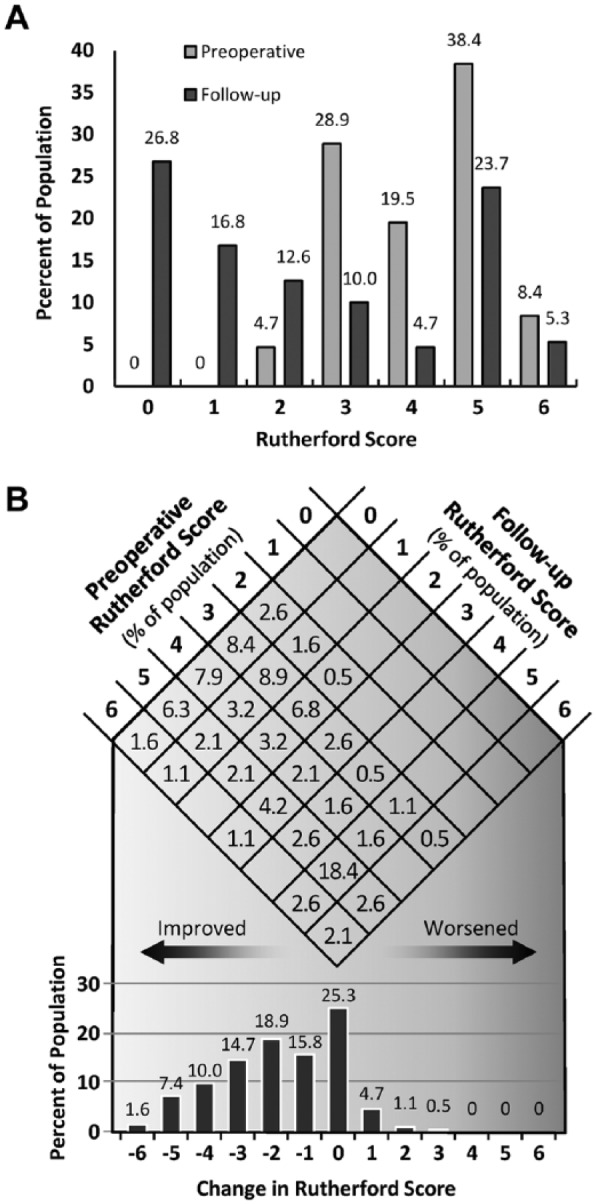
Methods: Twelve sites around the world prospectively enrolled 197 patients (mean age 71±11 years, range 41-93; 129 men) from May 2012 to July 2013 who met the inclusion criterion of at least one CTO for which a retrograde crossing procedure was planned or became necessary. The population consisted of 64 (32.5%) claudicants (Rutherford categories 2/3) and 133 (67.5%) patients with critical limb ischemia (Rutherford category ≥4). A primary antegrade attempt to cross had been made prior to the tibiopedal attempt in 132 (67.0%) cases. Techniques used for access, retrograde lesion crossing, and treatment were at the operator's discretion. Follow-up data were obtained 30 days after the procedure.
Results: Technical tibiopedal access success was achieved in 184 (93.4%) of 197 patients and technical occlusion crossing success in 157 (85.3%) of the 184 successful tibial accesses. Failed access attempts were more common in women (9 of 13 failures). The rate of successful crossing was roughly equivalent between sexes [84.7% (50/59) women compared to 85.6% (107/125) men]. Technical success did not differ significantly based on a prior failed antegrade attempt: the access success rate was 92.4% (122/132) after a failed antegrade access vs 95.4% (62/65) in those with a primary tibiopedal attempt (p=0.55). Similarly, crossing success was achieved in 82.8% (101/122) after a failed antegrade access vs 90.3% (56/62) for patients with no prior antegrade attempt (p=0.19). Minor complications related to the access site occurred in 11 (5.6%) cases; no patient had access vessel thrombosis, compartment syndrome, or surgical revascularization.
Conclusion: Tibiopedal access appears to be safe and can be used effectively for the crossing of infrainguinal lesions in patients with severe lower limb ischemia.
Keywords: chronic total occlusion; critical limb ischemia; peripheral artery disease; retrograde approach; tibiopedal; transpedal; vascular access.
© The Author(s) 2016.
Conflict of interest statement
Figures
Comment in
-
Commentary: Alternative Approach to Successful Crossing: The Retrograde Tibiopedal Technique.J Endovasc Ther. 2016 Dec;23(6):847-850. doi: 10.1177/1526602816665294. Epub 2016 Aug 24. J Endovasc Ther. 2016. PMID: 27558462 No abstract available.
References
-
- Iyer SS, Dorros G, Zaitoun R, et al. Retrograde recanalization of an occluded posterior tibial artery by using a posterior tibial cutdown: two case reports. Cathet Cardiovasc Diag. 1990;20:251–253. - PubMed
-
- Allie DE, Hebert CJ, Walker CM, et al. Critical limb ischemia: a global epidemic. A critical analysis of current treatment unmasks the clinical and economic costs of CLI. EuroIntervention. 2005;1:75–84. - PubMed
-
- Norgren L, Hiatt WR, Dormandy JA, et al. Inter-society consensus for the management of peripheral arterial disease (TASC II). J Vasc Surg. 2007;45(suppl S):S5–S67. - PubMed
-
- Montero-Baker M, Schmidt A, Bräunlich S, et al. Retrograde approach for complex popliteal and tibioperoneal occlusions. J Endovasc Ther. 2008;15:594–604. - PubMed
-
- Rogers RK, Dattilo PB, Garcia JA, et al. Retrograde approach to recanalization of complex tibial disease. Catheter Cardiovasc Interv. 2011;77:915–925. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
