

A Novel SCN5A Mutation Associated with Drug Induced Brugada Type ECG
- PMID: 27560382
- PMCID: PMC4999187
- DOI: 10.1371/journal.pone.0161872
A Novel SCN5A Mutation Associated with Drug Induced Brugada Type ECG
Abstract
Background: Class IC antiarrhythmic agents may induce acquired forms of Brugada Syndrome. We have identified a novel mutation in SCN5A, the gene that encodes the α-subunit of the human cardiac sodium channel (hNav1.5), in a patient who exhibited Brugada- type ECG changes during pharmacotherapy of atrial arrhythmias.
Objective: To assess whether the novel mutation p.V1328M can cause drug induced Brugada Syndrome.
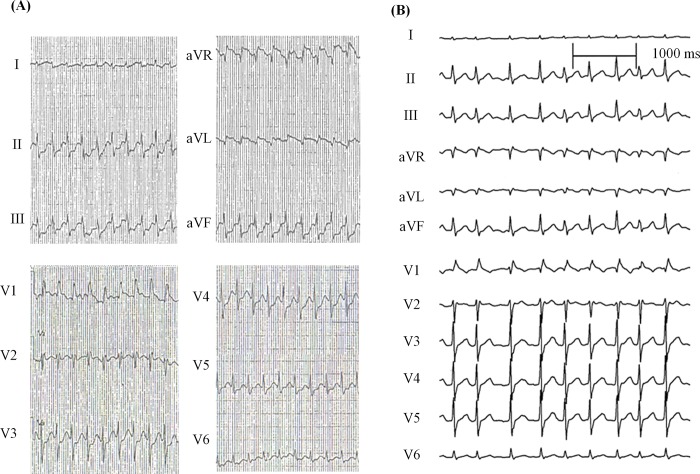
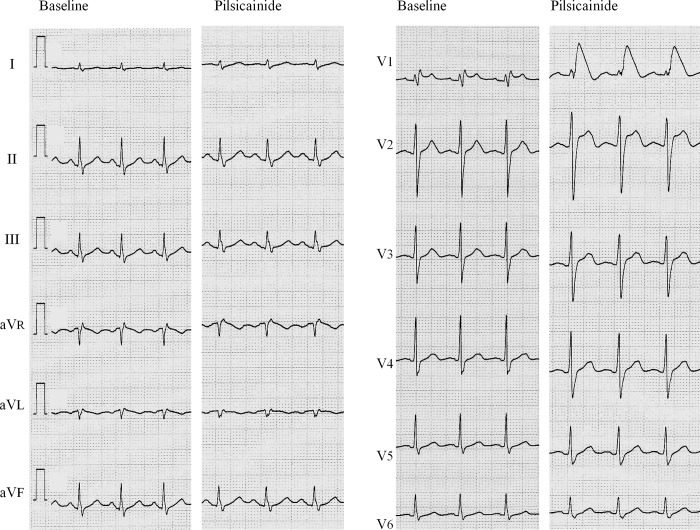
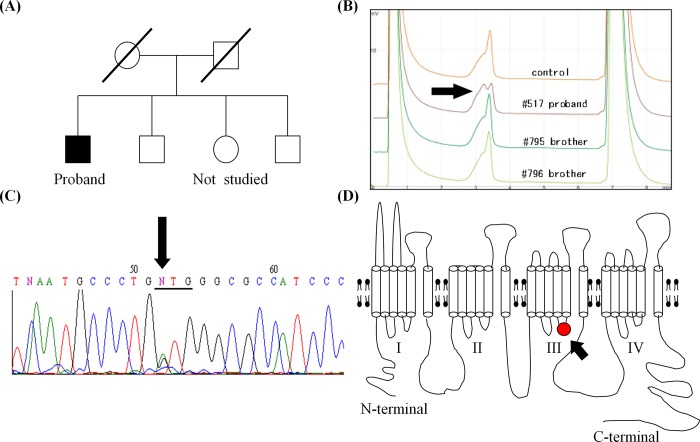
Methods: Administration of pilsicainide, a class IC antiarrhythmic agent, caused Brugada- type ST elevation in a 66-year-old Japanese male who presented with paroxysmal atrial fibrillation (PAF), type I atrial flutter and inducible ventricular fibrillation (VF) during electrophysiological study. Genetic screening using direct sequencing identified a novel SCN5A variant, p.V1328M. Electrophysiological parameters of WT and p.V1328M and their effects on drug pharmacokinetics were studied using the patch-clamp method.
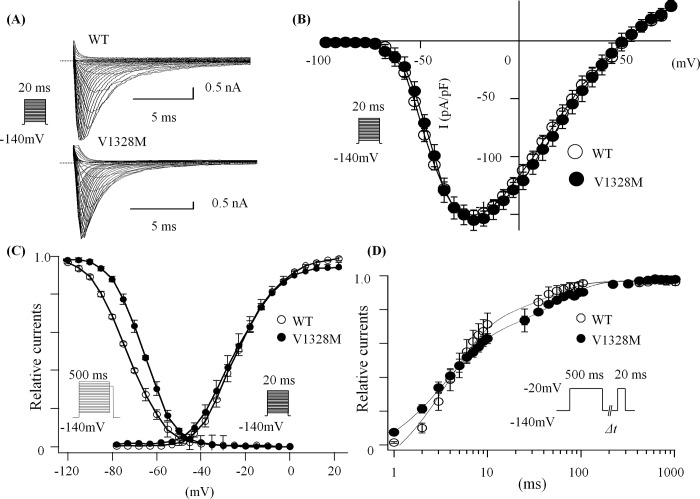
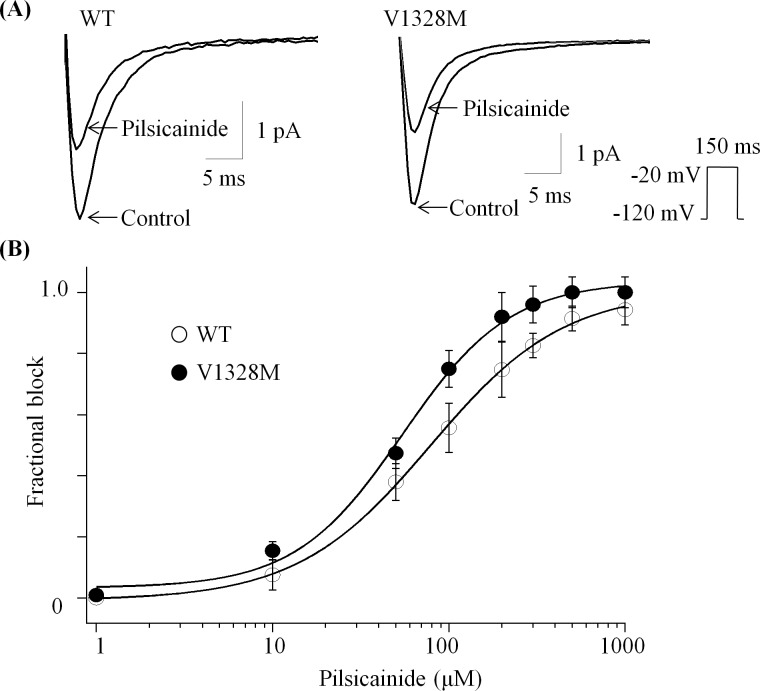
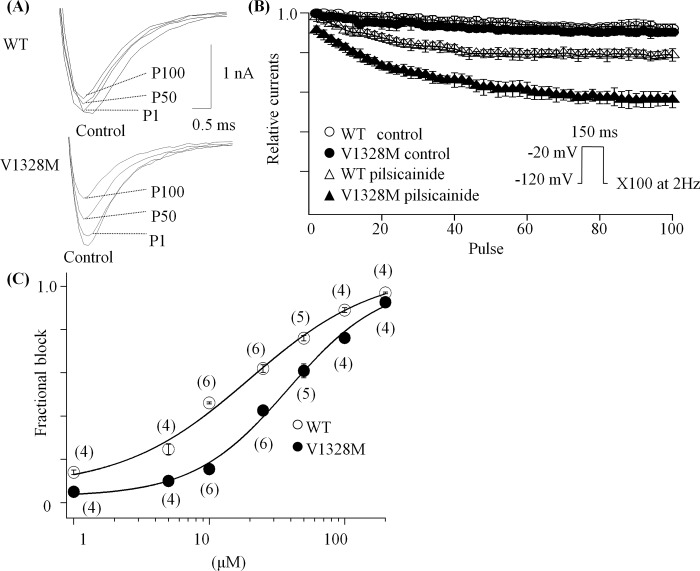
Results: Whole-cell sodium current densities were similar for WT and p.V1328M channels. While p.V1328M mutation did not affect the voltage-dependence of the activation kinetics, it caused a positive shift of voltage-dependent steady-state inactivation by 7 mV. The tonic block in the presence of pilsicainide was similar in WT and p.V1328M, when sodium currents were induced by a low frequency pulse protocol (q15s). On the contrary, p.V1328M mutation enhanced pilsicainide induced use-dependent block at 2 Hz. (Ki: WT, 35.8 μM; V1328M, 19.3 μM).
Conclusion: Our study suggests that a subclinical SCN5A mutation, p.V1328M, might predispose individuals harboring it to drug-induced Brugada Syndrome.
Conflict of interest statement
Pilsicainide was provided by Daiichi Sankyo LTD., Tokyo Japan. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Enhanced fast-inactivated state stability of cardiac sodium channels by a novel voltage sensor SCN5A mutation, R1632C, as a cause of atypical Brugada syndrome.Heart Rhythm. 2015 Nov;12(11):2296-304. doi: 10.1016/j.hrthm.2015.05.032. Epub 2015 May 29. Heart Rhythm. 2015. PMID: 26031372
-
Pilsicainide Administration Unmasks a Phenotype of Brugada Syndrome in a Patient with Overlap Syndrome due to the E1784K SCN5A Mutation.Intern Med. 2020 Jan 1;59(1):83-87. doi: 10.2169/internalmedicine.3430-19. Epub 2019 Sep 3. Intern Med. 2020. PMID: 31484910 Free PMC article.
-
Lidocaine-induced Brugada syndrome phenotype linked to a novel double mutation in the cardiac sodium channel.Circ Res. 2008 Aug 15;103(4):396-404. doi: 10.1161/CIRCRESAHA.108.172619. Epub 2008 Jul 3. Circ Res. 2008. PMID: 18599870 Free PMC article.
-
[Doubts of the cardiologist regarding an electrocardiogram presenting QRS V1-V2 complexes with positive terminal wave and ST segment elevation. Consensus Conference promoted by the Italian Cardiology Society].G Ital Cardiol (Rome). 2010 Nov;11(11 Suppl 2):3S-22S. G Ital Cardiol (Rome). 2010. PMID: 21361048 Italian.
-
The Brugada syndrome.Acta Cardiol. 2009 Dec;64(6):795-801. doi: 10.2143/AC.64.6.2044745. Acta Cardiol. 2009. PMID: 20128157 Review.
Cited by
-
SCN5A variant type-dependent risk prediction in Brugada syndrome.Europace. 2025 Feb 5;27(2):euaf024. doi: 10.1093/europace/euaf024. Europace. 2025. PMID: 39931825 Free PMC article.
-
Dysfunctional Nav1.5 channels due to SCN5A mutations.Exp Biol Med (Maywood). 2018 Jun;243(10):852-863. doi: 10.1177/1535370218777972. Epub 2018 May 27. Exp Biol Med (Maywood). 2018. PMID: 29806494 Free PMC article. Review.
-
Drug-induced Brugada-type Electrocardiogram: A Cause of Sudden Death in Patients with Schizophrenia?Intern Med. 2017 Nov 15;56(22):2969-2970. doi: 10.2169/internalmedicine.9087-17. Epub 2017 Oct 16. Intern Med. 2017. PMID: 29033432 Free PMC article. No abstract available.
-
[Functional analysis of a novel SCN5A mutation G1712C identified in Brugada syndrome].Nan Fang Yi Ke Da Xue Xue Bao. 2016 Feb 20;37(2):256-260. doi: 10.3969/j.issn.1673-4254.2017.02.19. Nan Fang Yi Ke Da Xue Xue Bao. 2016. PMID: 28219873 Free PMC article. Chinese.
References
-
- Kumagai K, Nakashima H, Tojo H, Yasuda T, Noguchi H, Matsumoto N, et al. Pilsicainide for atrial fibrillation. Drugs. 2006;66(16):2067–73. - PubMed
-
- Hirose M, Ohkubo Y, Takano M, Hamazaki M, Sekido T, Yamada M. Mechanisms of the preventive effect of pilsicainide on atrial fibrillation originating from the pulmonary vein. Circulation journal: official journal of the Japanese Circulation Society. 2007;71(11):1805–14. - PubMed
-
- Nakazawa K, Sakurai T, Kishi R, Takagi A, Osada K, Ryu S, et al. Discrimination of Brugada syndrome patients from individuals with the saddle-back type ST-segment elevation using a marker of the standard 12-lead electrocardiography. Circulation journal: official journal of the Japanese Circulation Society. 2007;71(4):546–9. - PubMed
-
- Yodogawa K, Morita N, Kobayashi Y, Takayama H, Ohara T, Katoh T, et al. High-frequency potentials developed in wavelet-transformed electrocardiogram as a novel indicator for detecting Brugada syndrome. Heart rhythm: the official journal of the Heart Rhythm Society. 2006;3(12):1436–44. - PubMed
-
- Shimizu W. Acquired forms of the Brugada syndrome. Journal of electrocardiology. 2005;38(4 Suppl):22–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
