

Equality in Maternal and Newborn Health: Modelling Geographic Disparities in Utilisation of Care in Five East African Countries
- PMID: 27561009
- PMCID: PMC4999282
- DOI: 10.1371/journal.pone.0162006
Equality in Maternal and Newborn Health: Modelling Geographic Disparities in Utilisation of Care in Five East African Countries
Erratum in
-
Correction: Equality in Maternal and Newborn Health: Modelling Geographic Disparities in Utilisation of Care in Five East African Countries.PLoS One. 2016 Oct 6;11(10):e0164519. doi: 10.1371/journal.pone.0164519. eCollection 2016. PLoS One. 2016. PMID: 27711195 Free PMC article.
Abstract
Background: Geographic accessibility to health facilities represents a fundamental barrier to utilisation of maternal and newborn health (MNH) services, driving historically hidden spatial pockets of localized inequalities. Here, we examine utilisation of MNH care as an emergent property of accessibility, highlighting high-resolution spatial heterogeneity and sub-national inequalities in receiving care before, during, and after delivery throughout five East African countries.
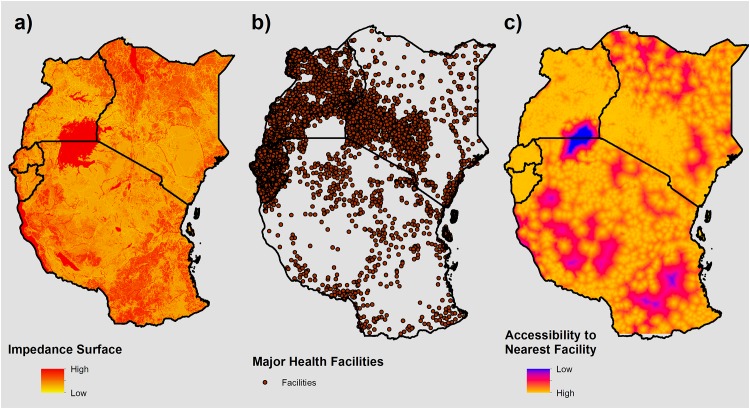
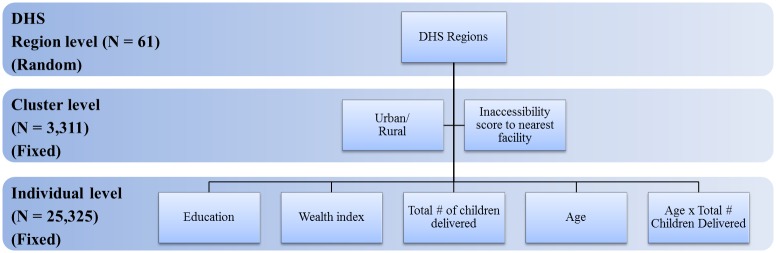
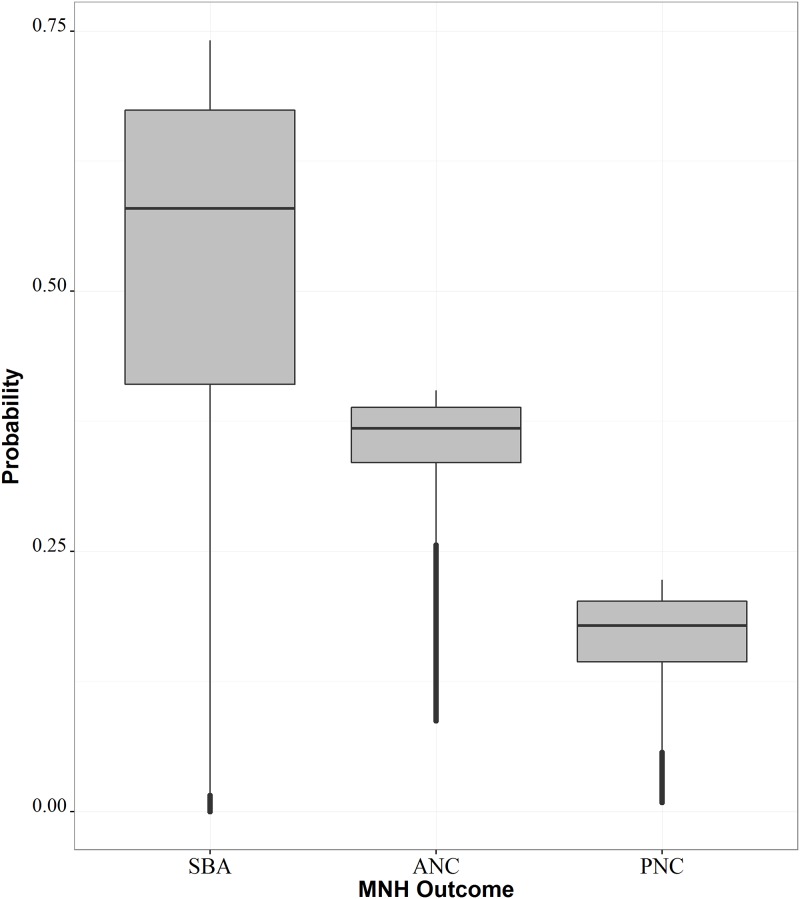
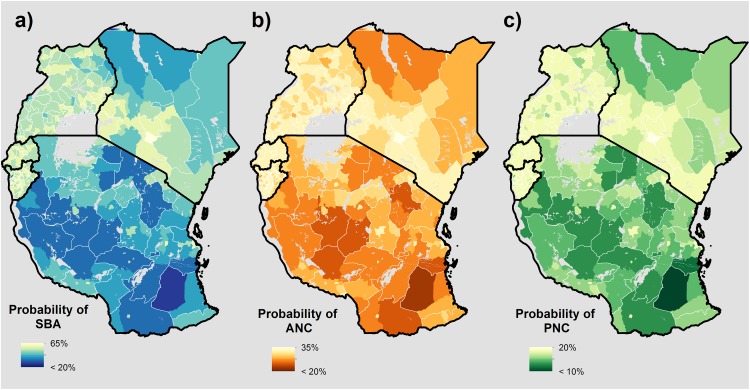
Methods: We calculated a geographic inaccessibility score to the nearest health facility at 300 x 300 m using a dataset of 9,314 facilities throughout Burundi, Kenya, Rwanda, Tanzania and Uganda. Using Demographic and Health Surveys data, we utilised hierarchical mixed effects logistic regression to examine the odds of: 1) skilled birth attendance, 2) receiving 4+ antenatal care visits at time of delivery, and 3) receiving a postnatal health check-up within 48 hours of delivery. We applied model results onto the accessibility surface to visualise the probabilities of obtaining MNH care at both high-resolution and sub-national levels after adjusting for live births in 2015.
Results: Across all outcomes, decreasing wealth and education levels were associated with lower odds of obtaining MNH care. Increasing geographic inaccessibility scores were associated with the strongest effect in lowering odds of obtaining care observed across outcomes, with the widest disparities observed among skilled birth attendance. Specifically, for each increase in the inaccessibility score to the nearest health facility, the odds of having skilled birth attendance at delivery was reduced by over 75% (0.24; CI: 0.19-0.3), while the odds of receiving antenatal care decreased by nearly 25% (0.74; CI: 0.61-0.89) and 40% for obtaining postnatal care (0.58; CI: 0.45-0.75).
Conclusions: Overall, these results suggest decreasing accessibility to the nearest health facility significantly deterred utilisation of all maternal health care services. These results demonstrate how spatial approaches can inform policy efforts and promote evidence-based decision-making, and are particularly pertinent as the world shifts into the Sustainable Goals Development era, where sub-national applications will become increasingly useful in identifying and reducing persistent inequalities.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Alkema L, Chou D, Hogan D, Zhang S, Moller A-B, Gemmill A, et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the UN Maternal Mortality Estimation Inter-Agency Group. The Lancet. 10.1016/S0140-6736(15)00838-7 - DOI - PMC - PubMed
-
- World Health Organization. State of inequality: Reproductive, maternal, newborn and child health. 2015. Available: http://apps.who.int/iris/bitstream/10665/164590/1/9789241564908_eng.pdf?...
-
- WHO | Maternal mortality. In: WHO. [cited 21 Dec 2015]. Available: http://www.who.int/mediacentre/factsheets/fs348/en/
-
- United Nations General Assembly. Transforming Our World: The 2030 Agenda for Sustainable Development. United Nations; 2015 Sep. Available: http://www.un.org/ga/search/view_doc.asp?symbol=A/RES/70/1
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
