

Increased sympathetic nerve activity and reduced cardiac baroreflex sensitivity in rheumatoid arthritis
- PMID: 27561790
- PMCID: PMC5285627
- DOI: 10.1113/JP272944
Increased sympathetic nerve activity and reduced cardiac baroreflex sensitivity in rheumatoid arthritis
Abstract
Key points: Rheumatoid arthritis (RA) is a chronic inflammatory condition associated with an increased risk of cardiovascular mortality. Increased sympathetic nerve activity and reduced cardiac baroreflex sensitivity heighten cardiovascular risk, althogh whether such autonomic dysfunction is present in RA is not known. In the present study, we observed an increased sympathetic nerve activity and reduced cardiac baroreflex sensitivity in patients with RA compared to matched controls. Pain was positively correlated with sympathetic nerve activity and negatively correlated with cardiac baroreflex sensitivity. The pattern of autonomic dysfunction that we describe may help to explain the increased cardiovascular risk in RA, and raises the possibility that optimizing pain management may resolve autonomic dysfunction in RA.
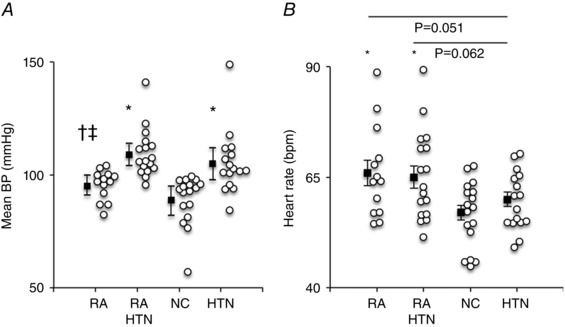
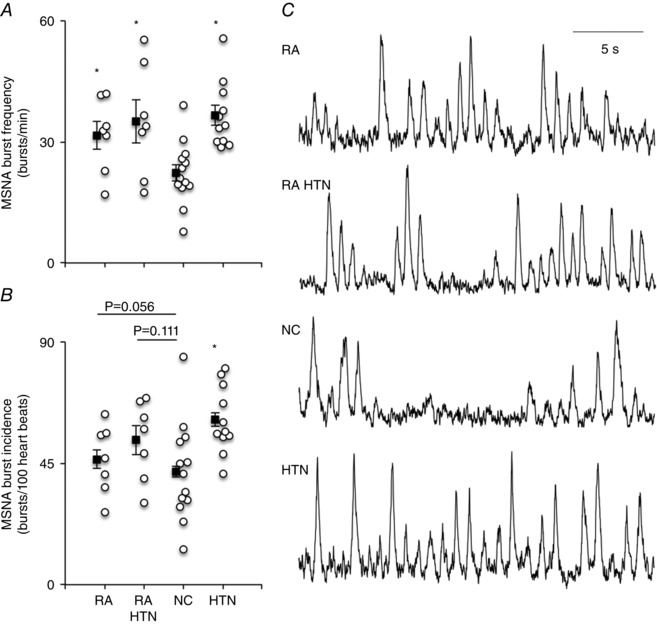
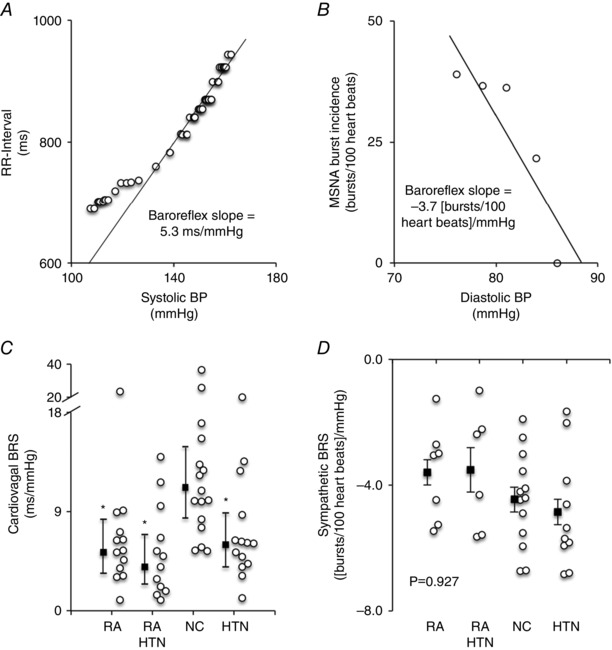
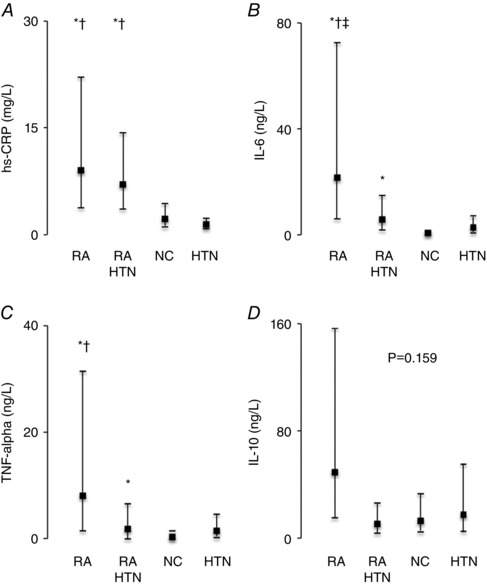
Abstract: Rheumatoid arthritis (RA) is a chronic inflammatory condition associated with increased cardiovascular morbidity/mortality and an incompletely understood pathophysiology. In animal studies, central and blood borne inflammatory cytokines that can be elevated in RA evoke pathogenic increases in sympathetic activity and reductions in baroreflex sensitivity (BRS). We hypothesized that muscle sympathetic nerve activity (MSNA) was increased and BRS decreased in RA. MSNA, blood pressure and heart rate (HR) were recorded in age- and sex-matched RA-normotensive (n = 13), RA-hypertensive patients (RA-HTN; n = 17), normotensive (NC; n = 17) and hypertensive controls (HTN; n = 16). BRS was determined using the modified Oxford technique. Inflammation and pain were determined using serum high sensitivity C-reactive protein (hs-CRP) and a visual analogue scale (VAS), respectively. MSNA was elevated similarly in RA, RA-HTN and HTN patients (32 ± 9, 35 ± 14, 37 ± 8 bursts min-1 ) compared to NC (22 ± 9 bursts min-1 ; P = 0.004). Sympathetic BRS was similar between groups (P = 0.927), whereas cardiac BRS (cBRS) was reduced in RA, RA-HTN and HTN patients [5(3-8), 4 (2-7), 6 (4-9) ms mmHg-1 ] compared to NC [11 (8-15) ms mmHg-1 ; P = 0.002]. HR was independently associated with hs-CRP. Increased MSNA and reduced cBRS were associated with hs-CRP although confounded in multivariable analysis. VAS was independently associated with MSNA burst frequency, cBRS and HR. We provide the first evidence for heightened sympathetic outflow and reduced cBRS in RA that can be independent of hypertension. In RA patients, reported pain was positively correlated with MSNA and negatively correlated with cBRS. Future studies should assess whether therapies to ameliorate pain and inflammation in RA restores autonomic balance and reduces cardiovascular events.
Keywords: autonomic nervous system; cytokine; inflammation; pain.
© 2016 The Authors. The Journal of Physiology published by John Wiley & Sons Ltd on behalf of The Physiological Society.
Figures
Comment in
-
Inflammation and cardiovascular autonomic dysfunction in rheumatoid arthritis: a bidirectional pathway leading to cardiovascular disease.J Physiol. 2017 Feb 15;595(4):1025-1026. doi: 10.1113/JP273649. J Physiol. 2017. PMID: 28198018 Free PMC article. No abstract available.
References
-
- Adlan AM, Lip GY, Paton JF, Kitas GD & Fisher JP (2014). Autonomic function and rheumatoid arthritis – a systematic review. Semin Arthritis Rheum 44, 283–304. - PubMed
-
- Amaya‐Amaya J, Sarmiento‐Monroy JC, Mantilla RD, Pineda‐Tamayo R, Rojas‐Villarraga A & Anaya JM (2013). Novel risk factors for cardiovascular disease in rheumatoid arthritis. Immunol Res 56, 267–286. - PubMed
-
- Arab HH & El‐Sawalhi MM (2013). Carvedilol alleviates adjuvant‐induced arthritis and subcutaneous air pouch edema: modulation of oxidative stress and inflammatory mediators. Toxicol Appl Pharmacol 268, 241–248. - PubMed
-
- Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS, Healey LA, Kaplan SR, Liang MH, Luthra HS & et al (1988). The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 31, 315–324. - PubMed
-
- Arosio E, De Marchi S, Rigoni A, Prior M, Delva P & Lechi A (2007). Forearm haemodynamics, arterial stiffness and microcirculatory reactivity in rheumatoid arthritis. J Hypertens 25, 1273–1278. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous