

The health and economic burden of bloodstream infections caused by antimicrobial-susceptible and non-susceptible Enterobacteriaceae and Staphylococcus aureus in European hospitals, 2010 and 2011: a multicentre retrospective cohort study
- PMID: 27562950
- PMCID: PMC4998424
- DOI: 10.2807/1560-7917.ES.2016.21.33.30319
The health and economic burden of bloodstream infections caused by antimicrobial-susceptible and non-susceptible Enterobacteriaceae and Staphylococcus aureus in European hospitals, 2010 and 2011: a multicentre retrospective cohort study
Abstract
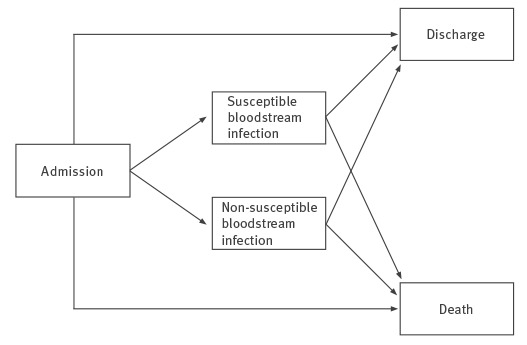
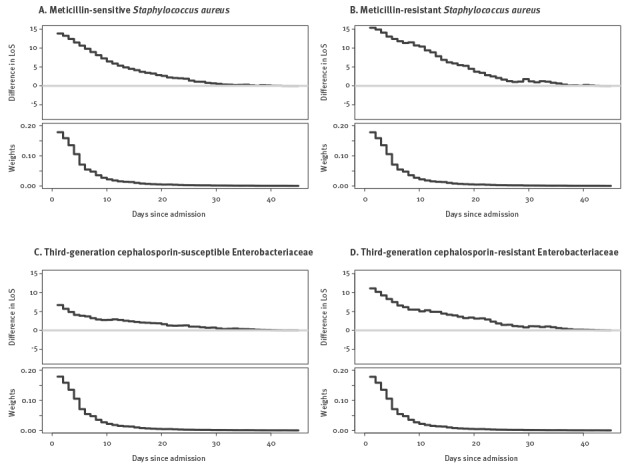
We performed a multicentre retrospective cohort study including 606,649 acute inpatient episodes at 10 European hospitals in 2010 and 2011 to estimate the impact of antimicrobial resistance on hospital mortality, excess length of stay (LOS) and cost. Bloodstream infections (BSI) caused by third-generation cephalosporin-resistant Enterobacteriaceae (3GCRE), meticillin-susceptible (MSSA) and -resistant Staphylococcus aureus (MRSA) increased the daily risk of hospital death (adjusted hazard ratio (HR) = 1.80; 95% confidence interval (CI): 1.34-2.42, HR = 1.81; 95% CI: 1.49-2.20 and HR = 2.42; 95% CI: 1.66-3.51, respectively) and prolonged LOS (9.3 days; 95% CI: 9.2-9.4, 11.5 days; 95% CI: 11.5-11.6 and 13.3 days; 95% CI: 13.2-13.4, respectively). BSI with third-generation cephalosporin-susceptible Enterobacteriaceae (3GCSE) significantly increased LOS (5.9 days; 95% CI: 5.8-5.9) but not hazard of death (1.16; 95% CI: 0.98-1.36). 3GCRE significantly increased the hazard of death (1.63; 95% CI: 1.13-2.35), excess LOS (4.9 days; 95% CI: 1.1-8.7) and cost compared with susceptible strains, whereas meticillin resistance did not. The annual cost of 3GCRE BSI was higher than of MRSA BSI. While BSI with S. aureus had greater impact on mortality, excess LOS and cost than Enterobacteriaceae per infection, the impact of antimicrobial resistance was greater for Enterobacteriaceae.
Keywords: Antimicrobial resistance; Escherichia coli; Meticillin-resistant Staphylococcus aureus (MRSA) in humans; Staphylococcus aureus; bacterial infections; bloodstream infection; multidrug resistance.
This article is copyright of The Authors, 2016.
Conflict of interest statement
HS is supported by research grants from The German Center for Infection Research (DZIF), the European Union (MagicBullet, Grant Agreement 278232), Novartis and Pfizer, has received speaking fees from Astellas, AstraZeneca, Gilead, MSD, Novartis, Oxoid and Pfizer, and is an advisory Board Member or consultant to AstraZeneca, Basilea, Cubist, FAB-Pharma, Novartis, SOBI, The Medicines Company, Theravance, and ThermoFischer. S. Hagel reports having received lecture fees from Pfizer, MSD, and Astra Zeneca. S. Harbarth reports having received investigator-initiated research grants funded by Pfizer and B. Braun; he is also a member of the advisory boards of Destiny Pharma, bioMerieux, Novartis and DaVolterra. Other authors: no conflicts to declare.
Figures
References
-
- World Health Organization (WHO). Antimicrobial resistance: global report on surveillance 2014. Geneva: WHO Press, 2014. Available from: http://www.who.int/drugresistance/documents/surveillancereport/en/
-
- Risks G. 2014. 9th edition. Geneva: World Economic Forum; 2014. Available from: http://reports.weforum.org/global-risks-2014/
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical