

Biology of Cholangiocytes: From Bench to Bedside
- PMID: 27563020
- PMCID: PMC5003190
- DOI: 10.5009/gnl16033
Biology of Cholangiocytes: From Bench to Bedside
Abstract
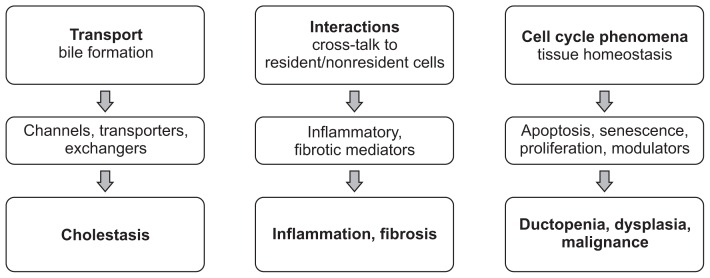
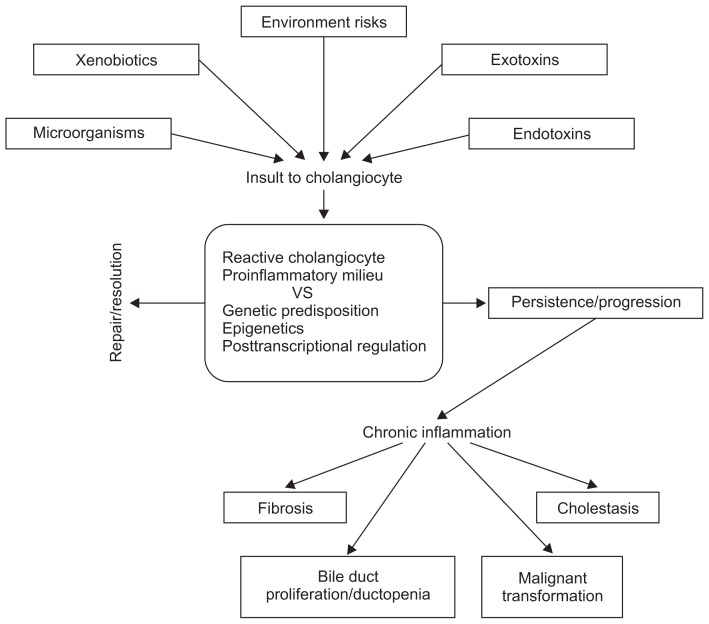
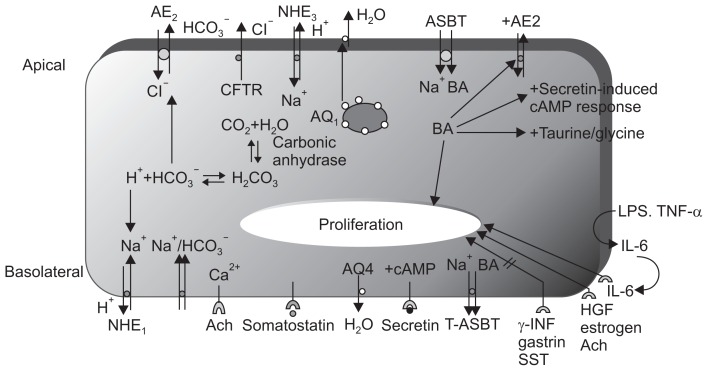
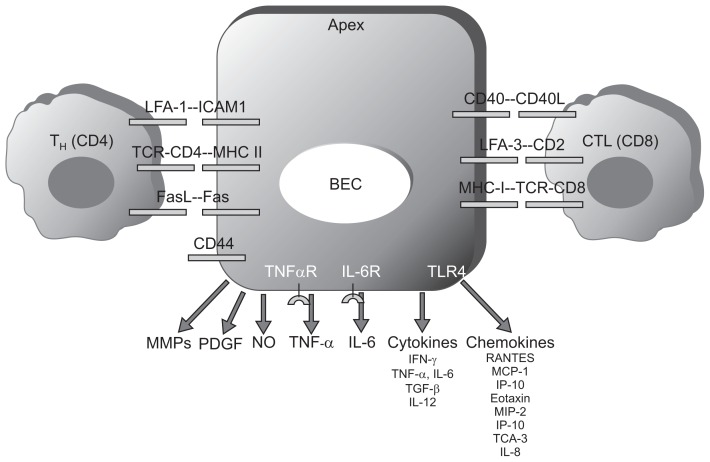
Cholangiocytes, the lining epithelial cells in bile ducts, are an important subset of liver cells. They are activated by endogenous and exogenous stimuli and are involved in the modification of bile volume and composition. They are also involved in damaging and repairing the liver. Cholangiocytes have many functions including bile production. They are also involved in transport processes that regulate the volume and composition of bile. Cholangiocytes undergo proliferation and cell death under a variety of conditions. Cholangiocytes have functional and morphological heterogenecity. The immunobiology of cholangiocytes is important, particularly for understanding biliary disease. Secretion of different proinflammatory mediators, cytokines, and chemokines suggests the major role that cholangiocytes play in inflammatory reactions. Furthermore, paracrine secretion of growth factors and peptides mediates extensive cross-talk with other liver cells, including hepatocytes, stellate cells, stem cells, subepithelial myofibroblasts, endothelial cells, and inflammatory cells. Cholangiopathy refers to a category of chronic liver diseases whose primary disease target is the cholangiocyte. Cholangiopathy usually results in end-stage liver disease requiring liver transplant. We summarize the biology of cholangiocytes and redefine the concept of cholangiopathy. We also discuss the recent progress that has been made in understanding the pathogenesis of cholangiopathy and how such progress has influenced therapy.
Keywords: Biology; Cholangiocyte; Cholangiopathy; Receptors; Transport.
Figures
References
-
- Strazzabosco M, Fabris L, Spirli C. Pathophysiology of cholangiopathies. J Clin Gastroenterol. 2005;39(4 Suppl 2):S90–S102. doi: 10.1097/01.mcg.0000155549.29643.ad. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
