

Unchanged pediatric out-of-hospital cardiac arrest incidence and survival rates with regional variation in North America
- PMID: 27565862
- PMCID: PMC5037038
- DOI: 10.1016/j.resuscitation.2016.07.244
Unchanged pediatric out-of-hospital cardiac arrest incidence and survival rates with regional variation in North America
Abstract
Aim: Outcomes for pediatric out-of-hospital cardiac arrest (OHCA) are poor. Our objective was to determine temporal trends in incidence and mortality for pediatric OHCA.
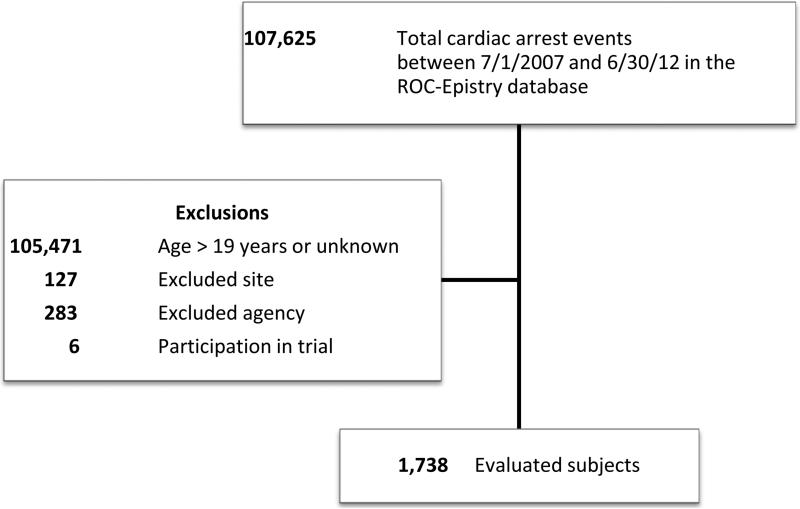
Methods: Adjusted incidence and hospital mortality rates of pediatric non-traumatic OHCA patients from 2007-2012 were analyzed using the 9 region Resuscitation Outcomes Consortium-Epidemiological Registry (ROC-Epistry) database. Children were divided into 4 age groups: perinatal (<3 days), infants (3days-1year), children (1-11 years), and adolescents (12-19 years). ROC regions were analyzed post-hoc.
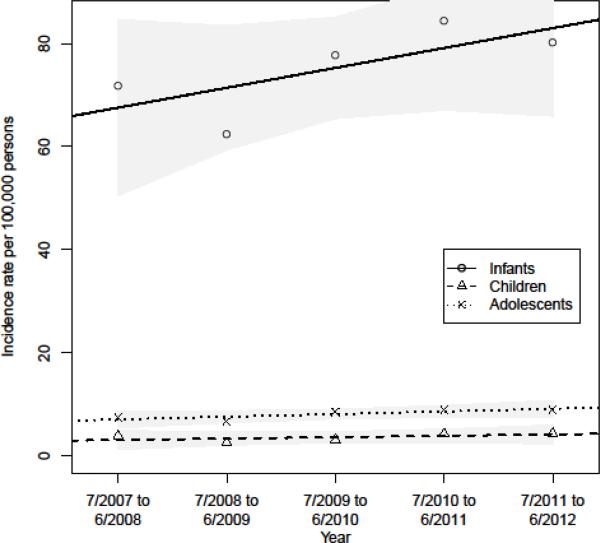
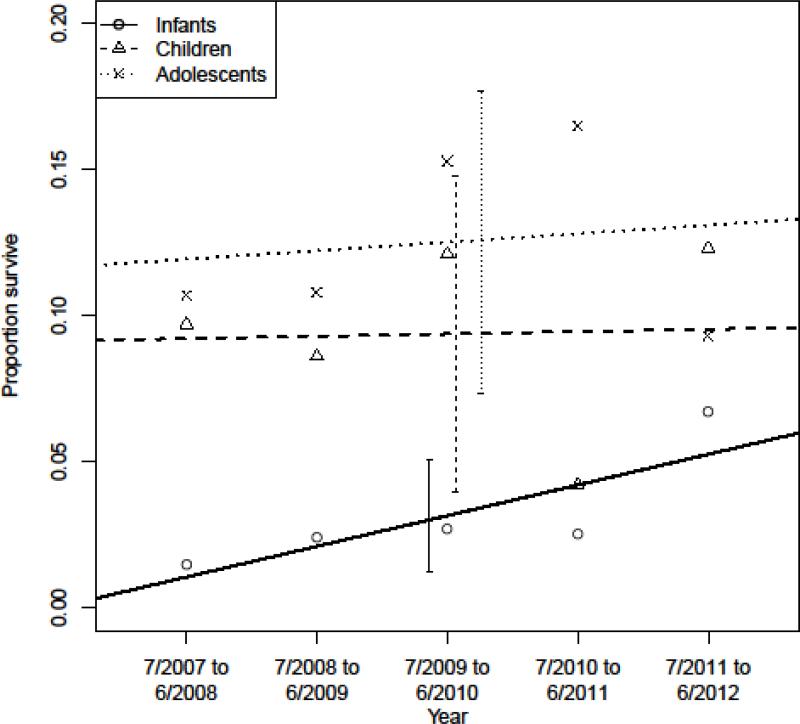
Results: We studied 1738 children with OHCA. The age- and sex-adjusted incidence rate of OHCA was 8.3 per 100,000 person-years (75.3 for infants vs. 3.7 for children and 6.3 for adolescents, per 100,000 person-years, p<0.001). Incidence rates differed by year (p<0.001) without overall linear trend. Annual survival rates ranged from 6.7-10.2%. Survival was highest in the perinatal (25%) and adolescent (17.3%) groups. Stratified by age group, survival rates over time were unchanged (all p>0.05) but there was a non-significant linear trend (1.3% increase) in infants. In the multivariable logistic regression analysis, infants, unwitnessed event, initial rhythm of asystole, and region were associated with worse survival, all p<0.001. Survival by region ranged from 2.6-14.7%. Regions with the highest survival had more cases of EMS-witnessed OHCA, bystander CPR, and increased EMS-defibrillation (all p<0.05).
Conclusions: Overall incidence and survival of children with OHCA in ROC regions did not significantly change over a recent 5year period. Regional variation represents an opportunity for further study to improve outcomes.
Keywords: Cardiac arrest; Epidemiology; Outcomes; Pediatric; Resuscitation.
Copyright © 2016 Elsevier Ireland Ltd. All rights reserved.
Figures
References
-
- Young KD, Gausche-Hill M, McClung CD, Lewis RJ. A prospective, population-based study of the epidemiology and outcome of out-of-hospital pediatric cardiopulmonary arrest. Pediatrics. 2004;114:157–64. - PubMed
-
- Del Castillo J, Lopez-Herce J, Matamoros M, et al. Hyperoxia, hypocapnia and hypercapnia as outcome factors after cardiac arrest in children. Resuscitation. 2012;83:1456–61. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
