

A comparative analysis of the effects of sevoflurane and propofol on cerebral oxygenation during steep Trendelenburg position and pneumoperitoneum for robotic-assisted laparoscopic prostatectomy
- PMID: 27565964
- PMCID: PMC5097119
- DOI: 10.1007/s00540-016-2241-y
A comparative analysis of the effects of sevoflurane and propofol on cerebral oxygenation during steep Trendelenburg position and pneumoperitoneum for robotic-assisted laparoscopic prostatectomy
Abstract
Purpose: Steep Trendelenburg position and pneumoperitoneum during robotic-assisted laparoscopic prostatectomy (RALP) increase intracranial pressure (ICP) and may alter cerebral blood flow (CBF) and oxygenation. Volatile anesthetics and propofol have different effects on ICP, CBF, and cerebral metabolic rate and may have different impact on cerebral oxygenation during RALP. In this study, we measured jugular venous bulb oxygenation (SjO2) and regional oxygen saturation (SctO2) in patients undergoing RALP to evaluate cerebral oxygenation and compared the effects of sevoflurane and propofol. We also verified whether SctO2 may be an alternative to SjO2.
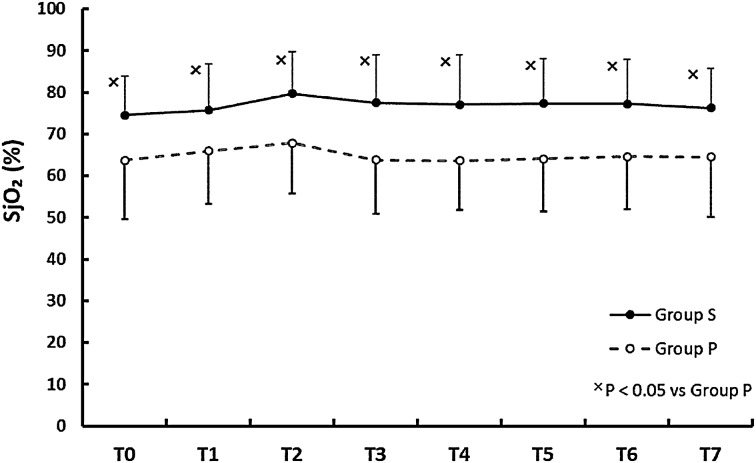
Methods: Fifty patients scheduled for RALP were randomly assigned to undergo sevoflurane (group S) or propofol (group P) anesthesia. SjO2, SctO2, mean arterial pressure (MAP), heart rate (HR), cardiac index (CI), central venous pressure (CVP), partial pressures of arterial oxygen (PaO2) and carbon dioxide (PaCO2), hemoglobin concentration (Hb), Bispectral Index (BIS) and nasopharyngeal temperature (BT) were recorded 5 min before surgery commencement, 5 min after pneumoperitoneum, 5, 30, 60, 90, and 120 min after pneumoperitoneum in a Trendelenburg position, and after desufflation in a supine position.
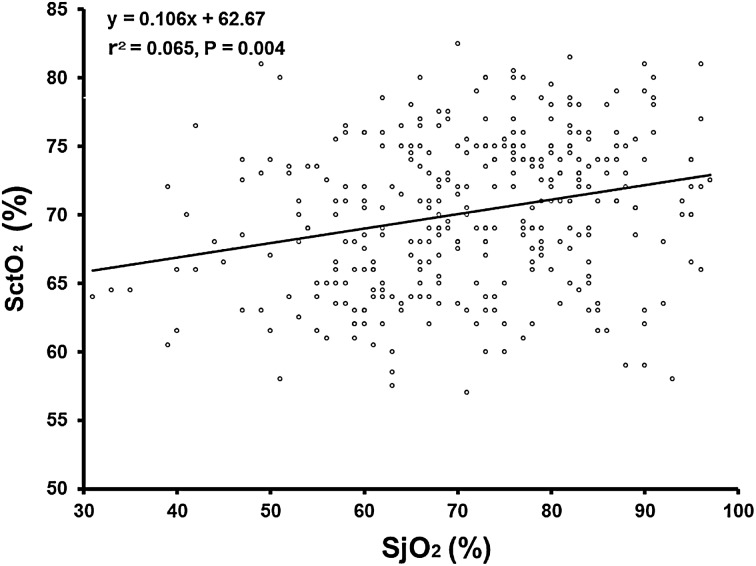
Results: SjO2 was significantly higher in group S than in group P at all measurement points [group S vs. group P: 77 % (11) vs. 65 % (13), mean of all measurement points (1SD); p < 0.01]. Linear regression analysis (β = 0.106; r 2 = 0.065; p = 0.004) shows a weak relationship between SjO2 and SctO2.
Conclusions: Sevoflurane maintains higher SjO2 levels than propofol during RALP. SctO2 does not accurately reflect SjO2.
Keywords: Cerebral oxygenation; Propofol; Robotic-assisted laparoscopic prostatectomy (RALP); Sevoflurane; Steep Trendelenburg position.
Conflict of interest statement
The authors declare no conflicts of interest associated with this manuscript.
Figures


References
-
- Dunham CM, Sosnowski C, Porter JM, Siegal J, Kohli C. Correlation of noninvasive cerebral oximetry with cerebral perfusion in the severe head injured patient: a pilot study. J Trauma. 2002;52:40–46. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
