

Abiraterone Acetate for the Treatment of Chemotherapy-Naïve Metastatic Castration-Resistant Prostate Cancer: An Evidence Review Group Perspective of an NICE Single Technology Appraisal
- PMID: 27566699
- PMCID: PMC5253156
- DOI: 10.1007/s40273-016-0445-5
Abiraterone Acetate for the Treatment of Chemotherapy-Naïve Metastatic Castration-Resistant Prostate Cancer: An Evidence Review Group Perspective of an NICE Single Technology Appraisal
Abstract
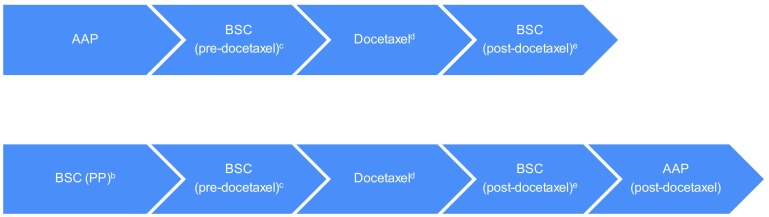
The National Institute for Health and Care Excellence (NICE) invited Janssen, the company manufacturing abiraterone acetate (AA; tradename Zytiga®), to submit evidence for the clinical and cost effectiveness of AA in combination with prednisone/prednisolone (AAP) compared with watchful waiting (i.e. best supportive care [BSC]) for chemotherapy-naïve patients with metastatic castration-resistant prostate cancer (mCRPC). Kleijnen Systematic Reviews Ltd (KSR), in collaboration with Maastricht University Medical Center, was commissioned as the Evidence Review Group (ERG). This paper presents a summary of the company submission (CS), the ERG report, subsequent addenda, and the development of the NICE guidance for the use of this drug in England and Wales by the Appraisal Committee (AC). The ERG produced a critical review of the clinical and cost effectiveness of AAP based on the CS. An important question in this appraisal was, according to the ERG, whether AAP followed by docetaxel is more effective than BSC followed by docetaxel. In the COU-AA-302 trial, 239 of 546 (43.8 %) AAP patients and 304 of 542 (56.1 %) BSC patients received docetaxel as subsequent therapy, following AA or placebo. The results for this specific group of patients were not presented in the CS; therefore, the ERG asked the company to provide these data in the clarification letter; however, these data were presented as commercial-in-confidence and cannot therefore be reported here. The ERG's critical assessment of the company's economic evaluation highlighted a number of concerns, including (a) not using the intention-to-treat (ITT) population; (b) inconsistencies in estimating prediction equations; (c) not fully incorporating the impact of adverse events; (d) incorrectly incorporating the new patient access scheme (PAS); and (e) the assumption that AA non-compliance leads to recoverable drug costs. Although some of these issues were adjusted in the ERG base case, the ERG could not estimate the impact of all of these issues, and thus acknowledges that there are still uncertainties concerning the cost-effectiveness evidence. With the exception of the ERG's preference for using the ITT population, the AC agreed with the approach taken in the ERG base case. The original company and ERG base-case incremental cost-effectiveness ratios (ICERs) were £46,722 and £57,688 per QALY gained, respectively; these changed to £28,563 and £38,061 per QALY gained, respectively, in the revised base cases applying a new PAS. Regarding the end-of-life criteria, after 24 months approximately 63 % of patients in the control group of the COU-AA-302 trial were still alive, and the median survival was 30.1 months (95 % CI 27.3-34.1). Therefore, it is unlikely that life expectancy would be less than 24 months. The AC stated that the most plausible ICER is likely between £28,600 and £32,800 per QALY gained, and concluded that AAP at this stage in the treatment pathway did not meet the end-of-life criterion for short life expectancy. Moreover, in March 2016, the AC produced the final guidance, stating that AAP is recommended, within its marketing authorisation, as an option for treating mCRPC.
Conflict of interest statement
Compliance with Ethical Standards Funding This project was funded by the National Institute for Health Research (NIHR) Health Technology Assessment (HTA) Programme (see the HTA programme website for further project information [http://www.hta.ac.uk]). This summary of the ERG report was compiled after NICE issued the FAD. The views and opinions expressed herein are those of the authors and do not necessarily reflect those of NICE or the Department of Health. Conflict of interest Bram Ramaekers, Rob Riemsma, Florian Tomini, Thea van Asselt, Sohan Deshpande, Steven Duffy, Nigel Armstrong, Johan Severens, Jos Kleijnen, and Manuela A. Joore have no conflicts of interest to declare. Contributions of authors All authors have commented on the submitted manuscript and have given their approval for the final version to be published. Rob Riemsma, Sohan Deshpande and Jos Kleijnen reviewed the clinical-effectiveness evidence; Steven Duffy reviewed the search methods; and Bram Ramaekers, Florian Tomini, Thea van Asselt, Nigel Armstrong, Johan Severens, and Manuela Joore reviewed the cost-effectiveness evidence. Bram Ramaekers acts as overall guarantor for the manuscript. This summary has not been externally peer reviewed by PharmacoEconomics.
Figures
Comment in
-
Comment on: "Abiraterone Acetate for the Treatment of Chemotherapy-Naïve Metastatic Castration-Resistant Prostate Cancer: An Evidence Review Group Perspective of an NICE Single Technology Appraisal".Pharmacoeconomics. 2017 Jun;35(6):661-663. doi: 10.1007/s40273-017-0502-8. Pharmacoeconomics. 2017. PMID: 28390016 No abstract available.
-
Response to Letter to the Editor Regarding "Abiraterone Acetate for the Treatment of Chemotherapy-Naïve Metastatic Castration-Resistant Prostate Cancer: An Evidence Review Group Perspective of a NICE Single Technology Appraisal".Pharmacoeconomics. 2017 Jun;35(6):665-667. doi: 10.1007/s40273-017-0507-3. Pharmacoeconomics. 2017. PMID: 28391508 No abstract available.
-
Cost-effectiveness of first-line hormone-therapies in chemonaïve castration-resistant prostate cancer Integrating the European Society for Medical Oncology Magnitude of Clinical Benefit Scale (ESMO-MCBS) with the costs of drugs.Recenti Prog Med. 2017 Jun;108(6):294-295. doi: 10.1701/2715.27717. Recenti Prog Med. 2017. PMID: 28631778 Italian. No abstract available.
References
-
- National Institute for Health and Care Excellence (NICE). Guide to the processes of technology appraisal. London: NICE; 2014. https://www.nice.org.uk/article/pmg19/chapter/foreword. Accessed 21 Mar 2016. - PubMed
-
- Janssen. Abiraterone acetate (Zytiga®) for the treatment of metastatic castration-resistant prostate cancer in men not previously treated with chemotherapy: submission to National Institute of Health and Clinical Excellence. Single technology appraisal (STA). Janssen; 2014.
-
- Riemsma R, Ramaekers BLT, Tomini F, Wolff R, van Asselt ADI, Joore MA, et al. Abiraterone for the treatment of chemotherapy naïve metastatic castration-resistant prostate cancer: a single technology appraisal. York: Kleijnen Systematic Reviews Ltd; 2014.
-
- National Institute for Health and Care Excellence (NICE). Abiraterone for treating metastatic hormone-relapsed prostate cancer before chemotherapy is indicated. London: NICE; 2016. https://www.nice.org.uk/guidance/TA387. Accessed 21 Mar 2016.
-
- National Institute for Health and Care Excellence (NICE). Abiraterone for castration-resistant metastatic prostate cancer previously treated with a docetaxel-containing regimen. London: NICE; 2012. https://www.nice.org.uk/guidance/ta259/history. Accessed 21 Mar 2016.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
