

Body Composition Remodeling and Mortality: The Health Aging and Body Composition Study
- PMID: 27567109
- PMCID: PMC5897837
- DOI: 10.1093/gerona/glw163
Body Composition Remodeling and Mortality: The Health Aging and Body Composition Study
Abstract
Background: Age-related losses of lean mass and shifts to central adiposity are related to functional decline and may predict mortality and/or explain part of the risk of weight loss. To determine how mortality risk is related to shifts in body composition, changes should be considered in the context of overall weight change.
Methods: Five-year changes in body composition were assessed with computed tomography (cm2) and dual x-ray absorptiometry (kg) in 869 men and 934 women initially aged 70-79 years. All-cause mortality was monitored for up to 12 years (2002-2003 to September 30, 2014), and risk was assessed using sex-specific Cox models.
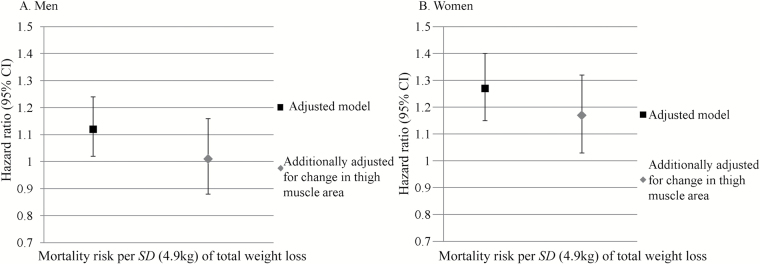
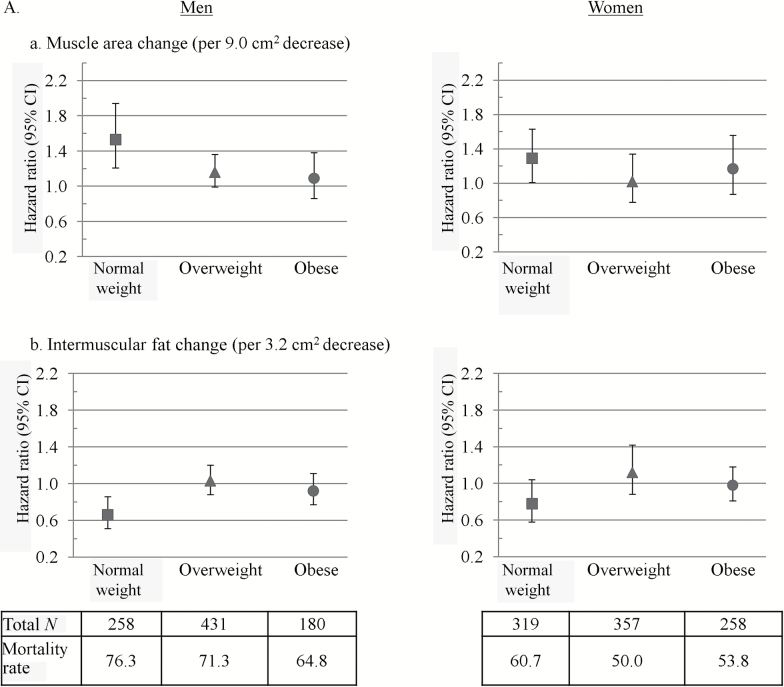
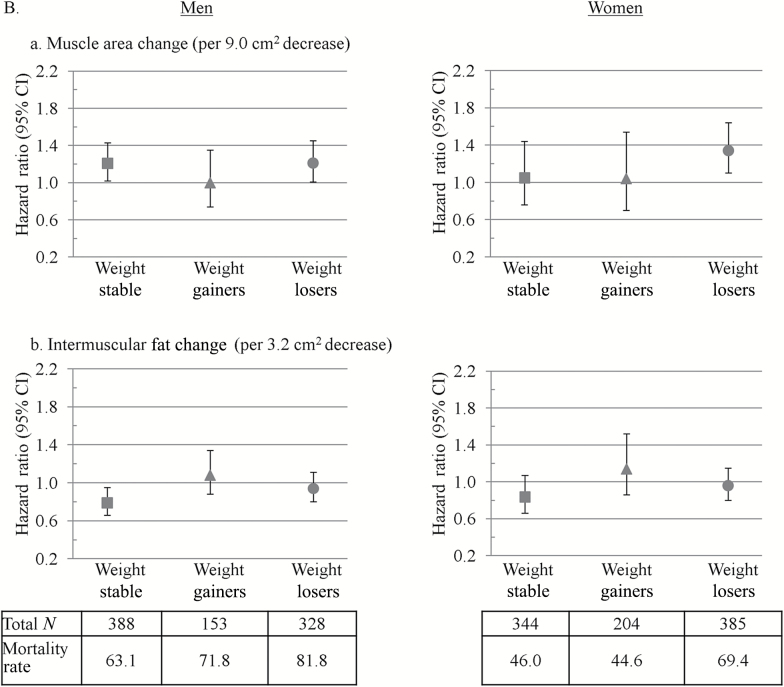
Results: Both men and women lost weight, visceral fat area, thigh muscle area, lean mass, and fat mass (all p < .01) but gained intermuscular thigh fat area (p < .01). There were 995 deaths. After adjustment for total weight change, demographics, and chronic disease, losing thigh muscle area was associated with higher mortality in both men (1.21, 1.08-1.35) and women (1.18, 1.01-1.37, per 9.0cm2) and was especially strong in normal weight (body mass index < 25kg/m2) individuals and those losing weight. Losing intermuscular thigh fat was protective against mortality only in normal weight (0.66, 0.51-0.86) and weight stable men (0.79, 0.66-0.95, per 3.2cm2). Changes in visceral fat area were not associated with mortality.
Conclusions: Older adults with greater loss of thigh muscle than expected for overall weight change had a higher mortality risk compared to those with relative thigh muscle preservation, suggesting that conservation of muscle mass is important for survival in old age.
Keywords: Body composition; Mortality; Muscle; Prospective cohort.
© The Author 2016. Published by Oxford University Press on behalf of The Gerontological Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Newman AB, Lee JS, Visser M, et al. Weight change and the conservation of lean mass in old age: the Health, Aging and Body Composition Study. Am J Clin Nutr. 2005;82:872–878; quiz 915. - PubMed
-
- Vlassopoulos A, Combet E, Lean ME. Changing distributions of body size and adiposity with age. Int J Obes (Lond). 2014;38:857–864. doi:10.1038/ijo.2013.216 - PubMed
-
- Newman AB, Kupelian V, Visser M, et al. ; Health ABC Study Investigators Sarcopenia: alternative definitions and associations with lower extremity function. J Am Geriatr Soc. 2003;51:1602–1609. doi:10.1046/j.1532-5415.2003.51534.x - PubMed
-
- Rolland Y, Gallini A, Cristini C, et al. Body-composition predictors of mortality in women aged ≥75 y: data from a large population-based cohort study with a 17-y follow-up. Am J Clin Nutr. 2014;100:1352–1360. doi:10.3945/ajcn.114.086728 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
