

Reviewing South Africa's malaria elimination strategy (2012-2018): progress, challenges and priorities
- PMID: 27567642
- PMCID: PMC5002155
- DOI: 10.1186/s12936-016-1497-x
Reviewing South Africa's malaria elimination strategy (2012-2018): progress, challenges and priorities
Abstract
Background: With a sustained national malaria incidence of fewer than one case per 1000 population at risk, in 2012 South Africa officially transitioned from controlling malaria to the ambitious goal of eliminating malaria within its borders by 2018. This review assesses the progress made in the 3 years since programme re-orientation while highlighting challenges and suggesting priorities for moving the malaria programme towards elimination.
Methods: National malaria case data and annual spray coverage data from 2010 until 2014 were assessed for trends. Information on surveillance, monitoring and evaluation systems, human and infrastructure needs and community malaria knowledge was sourced from the national programme mid-term review.
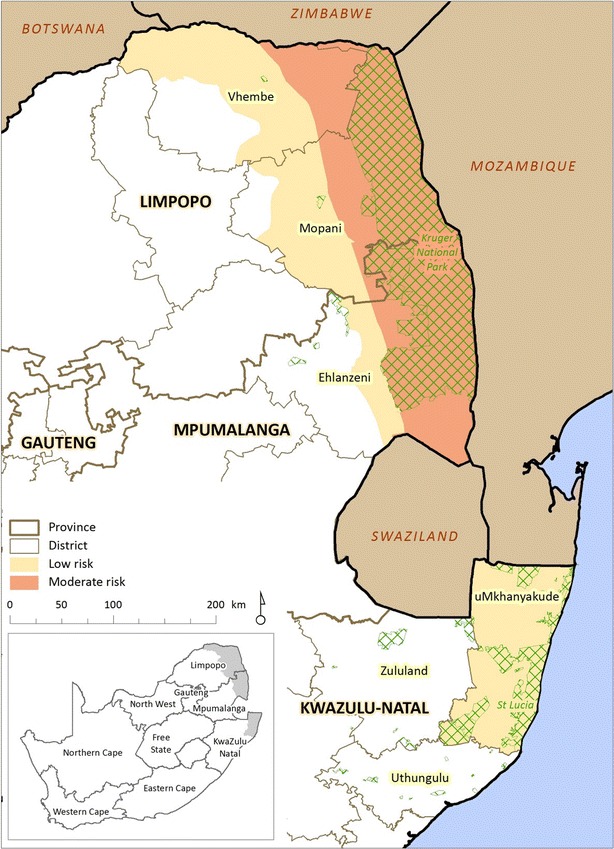
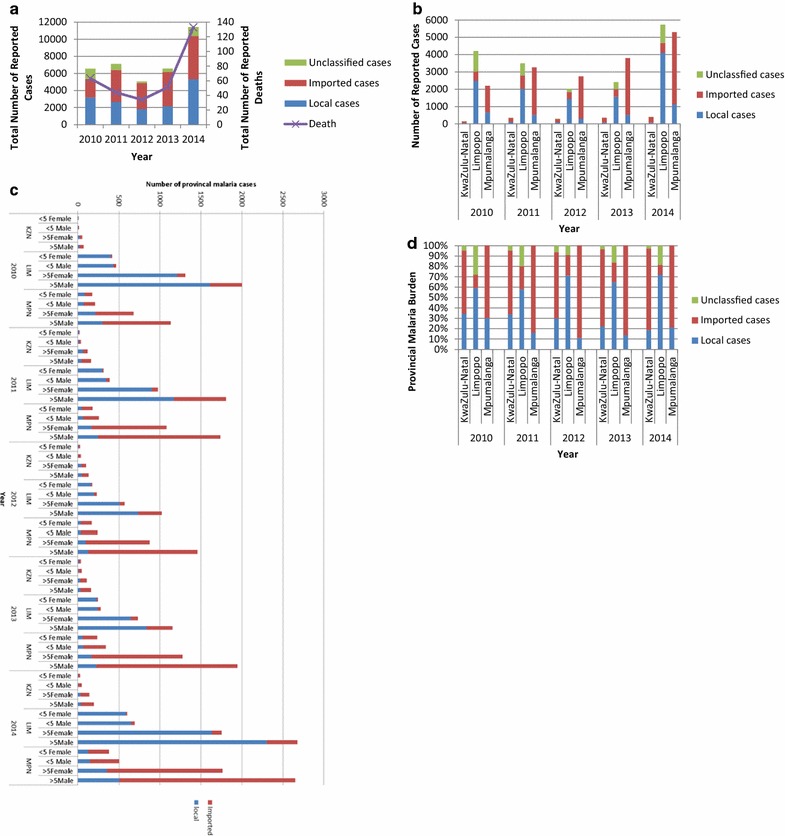
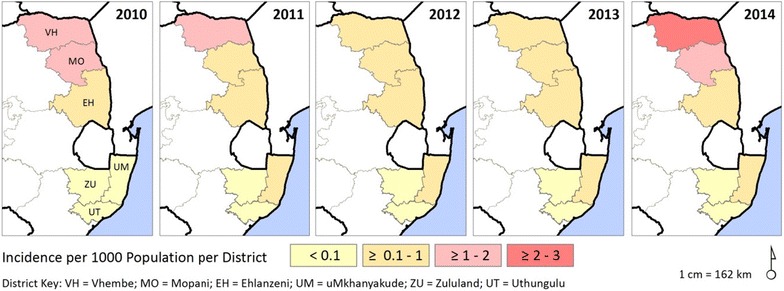
Results: Malaria cases increased markedly from 6811 in 2013 to 11,711 in 2014, with Mpumalanga and Limpopo provinces most affected. Enhanced local transmission appeared to drive malaria transmission in Limpopo Province, while imported malaria cases accounted for the majority of cases reported in Mpumalanga Province. Despite these increases only Vhembe and Mopani districts in Limpopo Province reported malaria incidences more than one case per 1000 population at risk by 2014. Over the review period annual spray coverage did not reach the recommended target of 90 % coverage, with information gaps identified in parasite prevalence, artemether-lumefantrine therapeutic utilization, asymptomatic/sub-patent carriage, drug efficacy, vector distribution and insecticide resistance.
Conclusions: Although South Africa has made steady progress since adopting an elimination agenda, a number of challenges have been identified. The heterogeneity of malaria transmission suggests interventions in Vhembe and Mopani districts should focus on control, while in KwaZulu-Natal Province eliminating transmission foci should be prioritized. Cross-border initiatives with neighbouring countries should be established/strengthened as a matter of urgency since malaria importation poses a real threat to the country's elimination efforts. It is also critical that provincial programmes are adequately resourced to effectively conduct the necessary targeted elimination activities, informed by current vector/parasite distribution and resistance data. More sensitive methods to detect sub-patent infections, primaquine as a transmission-blocking drug, and alternative vector control methods need to be investigated. Knowledge gaps among malaria health workers and affected communities should be identified and addressed.
Keywords: Case management; Challenges; Elimination; Malaria; Priorities; South Africa; Surveillance; Vector control.
Figures
References
-
- Hargreaves K, Koekemoer LL, Brooke BD, Hunt RH, Mthembu J, Coetzee M. Anopheles funestus resistant to pyrethroids in South Africa. Med Vet Entomol. 2000;103:793–798. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
