

Methoxyflurane Analgesia in Adult Patients in the Emergency Department: A Subgroup Analysis of a Randomized, Double-blind, Placebo-controlled Study (STOP!)
- PMID: 27567918
- PMCID: PMC5083764
- DOI: 10.1007/s12325-016-0405-7
Methoxyflurane Analgesia in Adult Patients in the Emergency Department: A Subgroup Analysis of a Randomized, Double-blind, Placebo-controlled Study (STOP!)
Abstract
Introduction: Acute pain remains highly prevalent in the Emergency Department (ED) setting. This double-blind, randomized, placebo-controlled UK study investigated the efficacy and safety of low-dose methoxyflurane analgesia for the treatment of acute pain in the ED in the adult population of the STOP! trial.
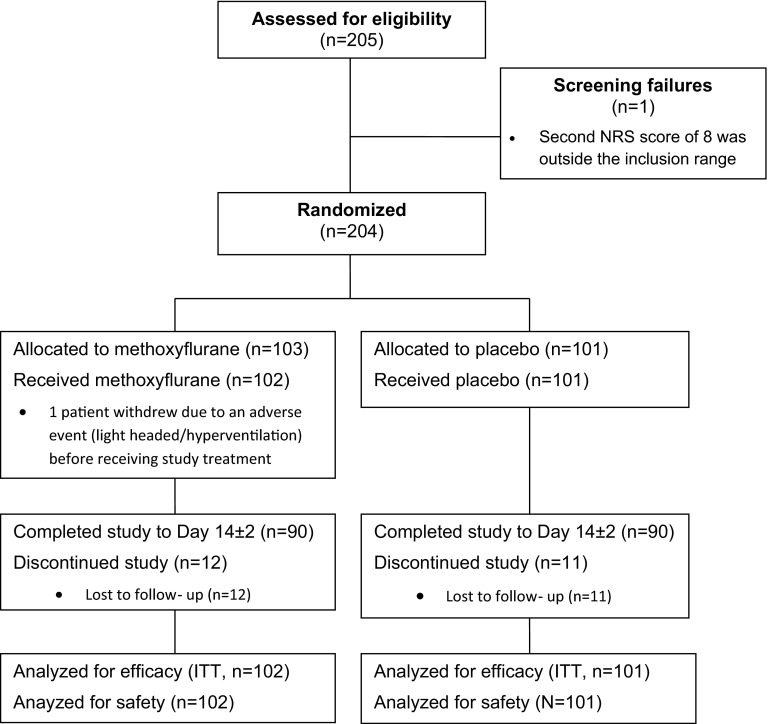
Methods: Patients presenting to the ED requiring analgesia for acute pain (pain score of 4-7 on the Numerical Rating Scale) due to minor trauma were randomized in a 1:1 ratio to receive methoxyflurane (up to 6 mL) or placebo (normal saline), both via a Penthrox® (Medical Developments International Limited, Scoresby, Australia) inhaler. Rescue medication (paracetamol/opioids) was available immediately upon request. Change from baseline in visual analog scale (VAS) pain intensity was the primary endpoint.
Results: 300 adult and adolescent patients were randomized; data are presented for the adult subgroup (N = 204). Mean baseline VAS pain score was ~66 mm in both groups. The mean change from baseline to 5, 10, 15 and 20 min was greater for methoxyflurane (-20.7, -27.4, -33.3 and -34.8 mm, respectively) than placebo (-8.0, -11.1, -12.3 and -15.2 mm, respectively). The primary analysis showed a highly significant treatment effect overall across all four time points (-17.4 mm; 95% confidence interval: -22.3 to -12.5 mm; p < 0.0001). Median time to first pain relief was 5 min with methoxyflurane [versus 20 min with placebo; (hazard ratio: 2.32; 95% CI: 1.63, 3.30; p < 0.0001)]; 79.4% of methoxyflurane-treated patients experienced pain relief within 1-10 inhalations. 22.8% of placebo-treated patients requested rescue medication within 20 min compared with 2.0% of methoxyflurane-treated patients (p = 0.0003). Methoxyflurane treatment was rated 'Excellent', 'Very Good' or 'Good' by 77.6% of patients, 74.5% of physicians and 72.5% of nurses. Treatment-related adverse events (mostly dizziness/headache) were reported by 42.2% of patients receiving methoxyflurane and 14.9% of patients receiving placebo; none caused withdrawal and the majority were mild and transient.
Conclusion: The results of this study support the evidence from previous trials that low-dose methoxyflurane administered via the Penthrox inhaler is a well-tolerated, efficacious and rapid-acting analgesic.
Funding: Medical Developments International (MDI) Limited and Mundipharma Research GmbH & Co.KG.
Trial registration: Clinicaltrials.gov identifier: NCT01420159, EudraCT number: 2011-000338-12.
Keywords: Acute pain; Analgesic; Emergency Department; Inhaled analgesic; Methoxyflurane; Pain; Penthrox, pre-hospital; Trauma.
Figures
Similar articles
-
Inhaled methoxyflurane (Penthrox®) versus placebo for injury-associated analgesia in children-the MAGPIE trial (MEOF-002): study protocol for a randomised controlled trial.Trials. 2019 Jul 4;20(1):393. doi: 10.1186/s13063-019-3511-4. Trials. 2019. PMID: 31272493 Free PMC article.
-
Analgesic Efficacy, Practicality and Safety of Inhaled Methoxyflurane Versus Standard Analgesic Treatment for Acute Trauma Pain in the Emergency Setting: A Randomised, Open-Label, Active-Controlled, Multicentre Trial in Italy (MEDITA).Adv Ther. 2019 Nov;36(11):3030-3046. doi: 10.1007/s12325-019-01055-9. Epub 2019 Oct 12. Adv Ther. 2019. PMID: 31612359 Free PMC article. Clinical Trial.
-
Low-dose methoxyflurane analgesia in adolescent patients with moderate-to-severe trauma pain: a subgroup analysis of the STOP! study.J Pain Res. 2019 Feb 15;12:689-700. doi: 10.2147/JPR.S188675. eCollection 2019. J Pain Res. 2019. PMID: 30863141 Free PMC article.
-
Methoxyflurane: A Review in Trauma Pain.Clin Drug Investig. 2016 Dec;36(12):1067-1073. doi: 10.1007/s40261-016-0473-0. Clin Drug Investig. 2016. PMID: 27738897 Review.
-
Inhaled Analgesia in Dermatologic Settings: A Comprehensive Overview of Methoxyflurane.Skin Therapy Lett. 2024 Sep;29(5):1-9. Skin Therapy Lett. 2024. PMID: 39353178 Review.
Cited by
-
Multimodal oral analgesia for non-severe trauma patients: evaluation of a triage-nurse directed protocol combining methoxyflurane, paracetamol and oxycodone.Intern Emerg Med. 2019 Oct;14(7):1139-1145. doi: 10.1007/s11739-019-02147-8. Epub 2019 Jul 9. Intern Emerg Med. 2019. PMID: 31290084
-
A Review of the Burden of Trauma Pain in Emergency Settings in Europe.Pain Ther. 2018 Dec;7(2):179-192. doi: 10.1007/s40122-018-0101-1. Epub 2018 Jun 2. Pain Ther. 2018. PMID: 29860585 Free PMC article. Review.
-
Prospective, Multicentre Trial of Methoxyflurane for Acute Trauma-Related Pain in Helicopter Emergency Medical Systems and Hostile Environments: METEORA Protocol.Adv Ther. 2018 Nov;35(11):2081-2092. doi: 10.1007/s12325-018-0816-8. Epub 2018 Oct 29. Adv Ther. 2018. PMID: 30374805 Free PMC article. Clinical Trial.
-
Determination of equi-analgesic doses of inhaled methoxyflurane versus intravenous fentanyl using the cold pressor test in volunteers: a randomised, double-blinded, placebo-controlled crossover study.Br J Anaesth. 2021 May;126(5):1038-1045. doi: 10.1016/j.bja.2020.12.045. Epub 2021 Mar 4. Br J Anaesth. 2021. PMID: 33676727 Free PMC article. Clinical Trial.
-
Identifying values and preferences around the choice of analgesia for patients with acute trauma pain in emergency and prehospital settings: using group concept mapping methodology.BMJ Open. 2020 Mar 10;10(3):e031863. doi: 10.1136/bmjopen-2019-031863. BMJ Open. 2020. PMID: 32161154 Free PMC article.
References
-
- Ventafridda V, Saita L, Ripamonti C, De Conno F. WHO guidelines for the use of analgesics in cancer pain. Int J Tissue React. 1985;7:93–96. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
