

Bowel strangulation caused by massive intraperitoneal adhesion due to effective chemotherapy for multiple peritoneal metastases originating from descending colon cancer
- PMID: 27568034
- PMCID: PMC5035323
- DOI: 10.1007/s12328-016-0679-y
Bowel strangulation caused by massive intraperitoneal adhesion due to effective chemotherapy for multiple peritoneal metastases originating from descending colon cancer
Abstract
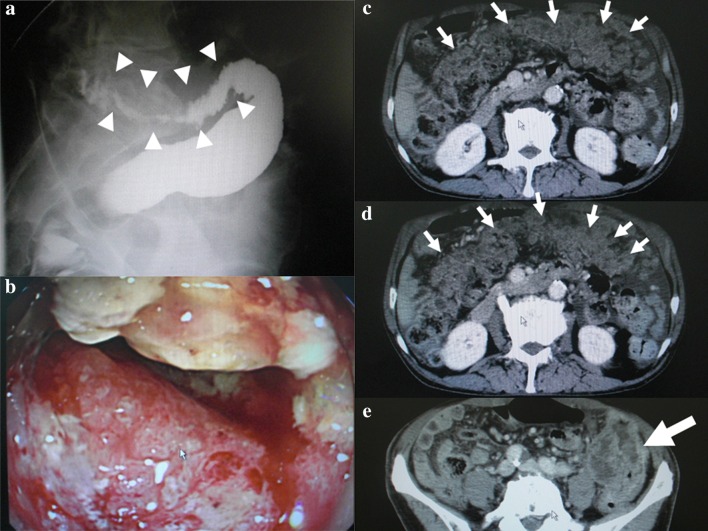
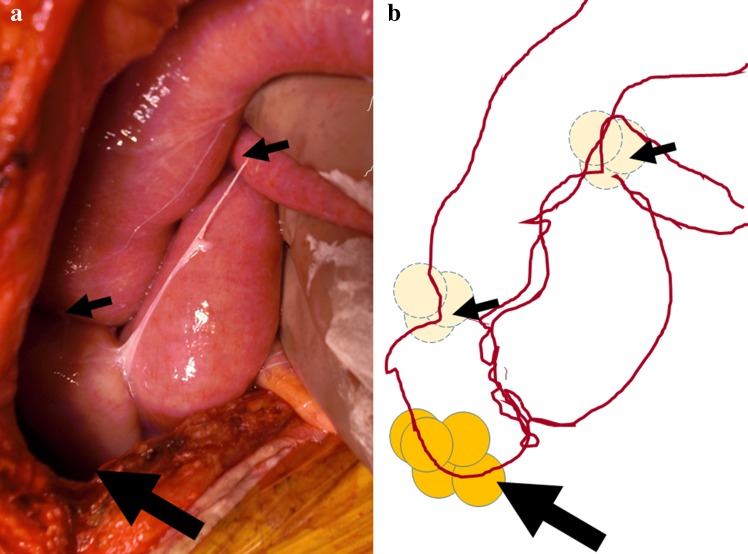
We describe a case of bowel strangulation caused by massive peritoneal adhesion as a result of effective chemotherapy. A 71-year-old man, who had obstructive descending colon cancer with massive peritoneal metastases and, therefore, received palliative surgery consisting of diverting colostomy and sampling of peritoneal nodules, developed bowel strangulation on day 4 of the 2nd course of chemotherapy, including irinotecan, l-leucovorin, and 5-fluorouracil. Emergent celiotomy showed a massive intraperitoneal adhesion formed around several intestinal loops, which were not observed at the prior surgery. One loop was strangled, but recovered by adhesiotomy alone. Intestinal loops were formed around aggregates of peritoneal nodules as the centers, several of which were then sampled. We closed the abdomen after all intestinal loops were eradicated by total enterolysis. Fortunately, the patient has been doing well and received chemotherapy without recurrent bowel obstruction 10 months after the present episode. Histological findings of the aggregates causing intestinal loops demonstrated extensive necrosis of cancerous tissue surrounded by fibrosis with abundant lymphocyte infiltration. These findings were not observed in the specimen sampled before chemotherapy, suggesting that intestinal loops were caused by inflammatory adhesion occurring around the peritoneal metastases as a result of effectiveness of chemotherapy.
Keywords: Adhesion; Chemotherapy; Colorectal cancer; Peritoneal dissemination; Strangulated ileus.
Conflict of interest statement
Compliance with ethical standards Conflict of Interest: The authors declare that they have no competing interests. Human Rights: All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Informed Consent: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. Institutional Review Board of the authors’ institution approved this manuscript for publication. A copy of the written consent is available for review by the Editor-in-Chief of this journal. Funding source: We have no funding source for this article.
Figures


Similar articles
-
[A case of juvenile colon cancer with peritoneal dissemination treated effectively by use of resection and chemotherapy].Gan To Kagaku Ryoho. 2014 Nov;41(12):1695-7. Gan To Kagaku Ryoho. 2014. PMID: 25731299 Review. Japanese.
-
[Systemic chemotherapy and surgery for recurrent metachronous liver metastases with peritoneal dissemination from triple colon cancers-a case report].Gan To Kagaku Ryoho. 2014 Dec;41(13):2615-7. Gan To Kagaku Ryoho. 2014. PMID: 25596059 Japanese.
-
[A case of advanced descending colon cancer with peritoneal dissemination responding to weekly high-dose l-leucovorin/5-fluorouracil combination therapy].Gan To Kagaku Ryoho. 2004 Jul;31(7):1105-8. Gan To Kagaku Ryoho. 2004. PMID: 15272595 Japanese.
-
[Super-elderly colon cancer with peritoneal dissemination effectively treated with modified FOLFOX6 chemotherapy--report of a case].Gan To Kagaku Ryoho. 2008 Nov;35(11):1955-7. Gan To Kagaku Ryoho. 2008. PMID: 19011351 Japanese.
-
[Novel approved form of treatment for colonic cancer with peritoneal metastases - radicality-aimed surgery combined with hyperthermic intraperitoneal chemotherapy].Duodecim. 2016;132(10):912-6. Duodecim. 2016. PMID: 27382828 Review. Finnish.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
