

Pregnancy and acromegaly
- PMID: 27568329
- PMCID: PMC5334433
- DOI: 10.1007/s11102-016-0740-3
Pregnancy and acromegaly
Abstract
Introduction: Acromegaly is a rare disorder in which, due to the high incidence of secondary hypogonadism, pregnancies are relatively rare. However, some women with acromegaly do get pregnant, which brings along questions about medication, complications and follow-up. This review tries to address these issues and provide the reader with practical information.
Methods: This review summarizes published data.
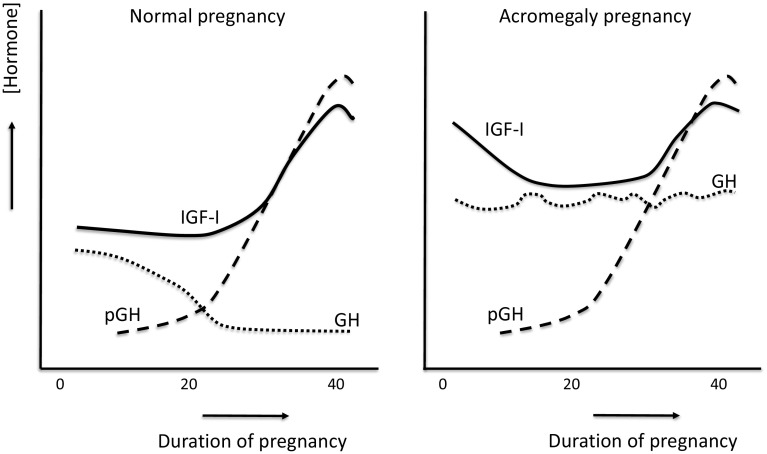
Conclusions: Acromegaly is a disorder that is characterized by changes in growth hormone (GH), insulin-like growth factor-1 (IGF-1) and insulin concentrations and actions. All these hormones are important in pregnancy as well. In principle, the fetal-placental collaboration between mother and child more-or-less takes over the control over GH and IGF-1, not only in normal physiology but also to a certain extend in acromegaly. When medication for the high GH levels or actions is continued during pregnancy, both dopamine agonists, somatostatin analogs and GH receptor antagonists have been used and the available data suggest that there are no adverse consequences on mother or fetus to date. However, it is strongly advised to stop any medical intervention during pregnancy until more data are available on the safety of these compounds. Also, medical treatment is not needed as tumor size and disease activity are not reported to escape.
Keywords: Acromegaly; Complications; Pregnancy; Review; Treatment.
Conflict of interest statement
A.M. has nothing to disclose, S.N. and A.J.vdL. have received speakers- and/or consultancy fees from Ipsen, Novartis and Pfizer.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
