

Association Between Quality Measures and Mortality in Individuals With Co-Occurring Mental Health and Substance Use Disorders
- PMID: 27568504
- PMCID: PMC5004087
- DOI: 10.1016/j.jsat.2016.06.001
Association Between Quality Measures and Mortality in Individuals With Co-Occurring Mental Health and Substance Use Disorders
Abstract
Importance: Individuals with co-occurring mental and substance use disorders have increased rates of mortality relative to the general population. The relationship between measures of treatment quality and mortality for these individuals is unknown.
Objective: To examine the association between 5 quality measures and 12- and 24-month mortality.
Design, setting and participants: Retrospective cohort study of patients with co-occurring mental illness (schizophrenia, bipolar disorder, post-traumatic stress disorder and major depression) and substance use disorders who received care for these disorders paid for by the Veterans Administration between October 2006 and September 2007. Logistic regression models were used to examine the association between 12 and 24-month mortality and 5 patient-level quality measures, while risk-adjusting for patient characteristics. Quality measures included receipt of psychosocial treatment, receipt of psychotherapy, treatment initiation and engagement, and a measure of continuity of care. We also examined the relationship between number of diagnosis-related outpatient visits and mortality, and conducted sensitivity analyses to examine the robustness of our findings to an unobserved confounder.
Main outcomes measure: Mortality 12 and 24 months after the end of the observation period.
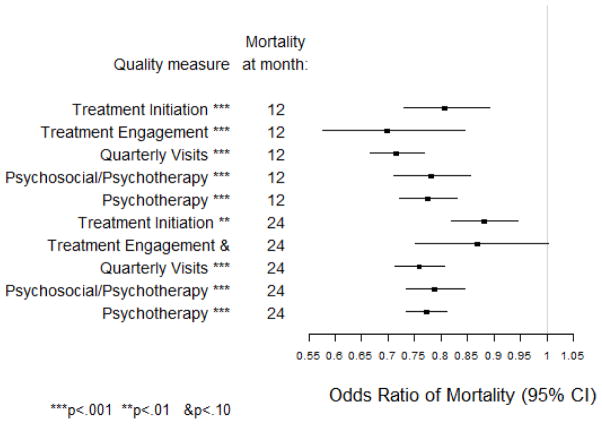
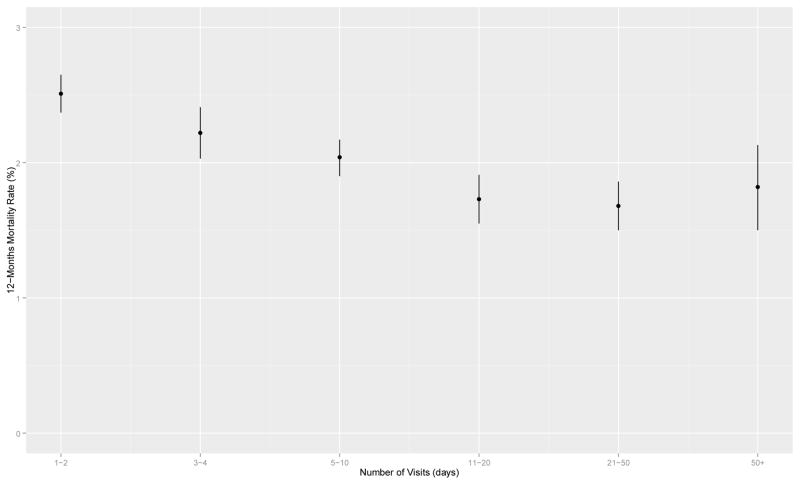
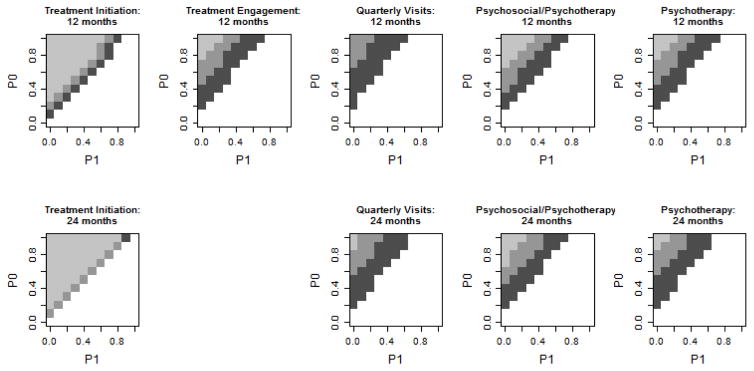
Results: All measures except for treatment engagement at 24 months were significantly associated with lower mortality at both 12 and 24 months. At 12 months, receiving any psychosocial treatment was associated with a 21% decrease in mortality; psychotherapy, a 22% decrease; treatment initiation, a 15% decrease, treatment engagement, a 31% decrease; and quarterly, diagnosis-related visits a 28% decrease. Increasing numbers of visits were associated with decreasing mortality. Sensitivity analyses indicated that the difference in the prevalence of an unobserved confounder would have to be unrealistically large given the observed data, or there would need to be a large effect of an unobserved confounder, to render these findings non-significant.
Conclusions and relevance: This is the first study to show an association between process-based quality measures and mortality in patients with co-occurring mental and substance use disorders, and provides initial support for the predictive validity of the measures. By devising strategies to improve performance on these measures, health care systems may be able to decrease the mortality of this vulnerable population.
Keywords: Co-occurring disorders; Mental health services; Mortality; Quality measures; Quality of care; Veterans.
Copyright © 2016 Elsevier Inc. All rights reserved.
Conflict of interest statement
none
Figures
Similar articles
-
Association between process measures and mortality in individuals with opioid use disorders.Drug Alcohol Depend. 2017 Aug 1;177:307-314. doi: 10.1016/j.drugalcdep.2017.03.033. Epub 2017 Jun 27. Drug Alcohol Depend. 2017. PMID: 28662975 Free PMC article.
-
Association Between Quality Measures and Perceptions of Care Among Patients With Substance Use Disorders.Psychiatr Serv. 2017 Nov 1;68(11):1150-1156. doi: 10.1176/appi.ps.201600484. Epub 2017 Jul 3. Psychiatr Serv. 2017. PMID: 28669291
-
A national survey of care for persons with co-occurring mental and substance use disorders.Psychiatr Serv. 2001 Aug;52(8):1062-8. doi: 10.1176/appi.ps.52.8.1062. Psychiatr Serv. 2001. PMID: 11474052
-
Integrated treatment of co-occurring mental illness and addiction: clinical intervention, program, and system perspectives.CNS Spectr. 2004 Dec;9(12):892-904, 925. doi: 10.1017/s1092852900009718. CNS Spectr. 2004. PMID: 15618940 Review.
-
Co-occurring mental and substance use disorders: promising approaches and research issues.Subst Use Misuse. 2000 Oct-Dec;35(12-14):2061-93. doi: 10.3109/10826080009148250. Subst Use Misuse. 2000. PMID: 11138717 Review.
Cited by
-
Relational continuity may give better clinical outcomes in patients with serious mental illness - a systematic review.BMC Psychiatry. 2023 Dec 18;23(1):952. doi: 10.1186/s12888-023-05440-1. BMC Psychiatry. 2023. PMID: 38110889 Free PMC article.
-
Patient characteristics associated with treatment initiation and engagement among individuals diagnosed with alcohol and other drug use disorders in emergency department and primary care settings.Subst Abus. 2019;40(3):278-284. doi: 10.1080/08897077.2018.1547812. Epub 2019 Jan 31. Subst Abus. 2019. PMID: 30702983 Free PMC article.
-
Association between process measures and mortality in individuals with opioid use disorders.Drug Alcohol Depend. 2017 Aug 1;177:307-314. doi: 10.1016/j.drugalcdep.2017.03.033. Epub 2017 Jun 27. Drug Alcohol Depend. 2017. PMID: 28662975 Free PMC article.
-
Integration of pharmacotherapy for alcohol use disorder treatment in primary care settings: A scoping review.J Subst Abuse Treat. 2023 Jan;144:108919. doi: 10.1016/j.jsat.2022.108919. Epub 2022 Oct 28. J Subst Abuse Treat. 2023. PMID: 36332528 Free PMC article.
-
A scoping review of healthcare effectiveness data and information set (HEDIS) substance use disorder measures.Ann Med. 2025 Dec;57(1):2447413. doi: 10.1080/07853890.2024.2447413. Epub 2025 Jan 2. Ann Med. 2025. PMID: 39745202 Free PMC article.
References
-
- Centers for Disease Control and Prevention. Alcohol deaths. 2014 Retrieved February 12, 2016, from http://www.cdc.gov/features/alcohol-deaths/
-
- Charbonneau A, Rosen AK, Ash AS, Owen RR, Kader B, Spiro A, III, … Kazis L. Measuring the quality of depression care in a large integrated health system. Medical Care. 2003;41(5):669–680. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
