

Spread of Psoriasiform Inflammation to Remote Tissues Is Restricted by the Atypical Chemokine Receptor ACKR2
- PMID: 27568525
- PMCID: PMC5176004
- DOI: 10.1016/j.jid.2016.07.039
Spread of Psoriasiform Inflammation to Remote Tissues Is Restricted by the Atypical Chemokine Receptor ACKR2
Abstract
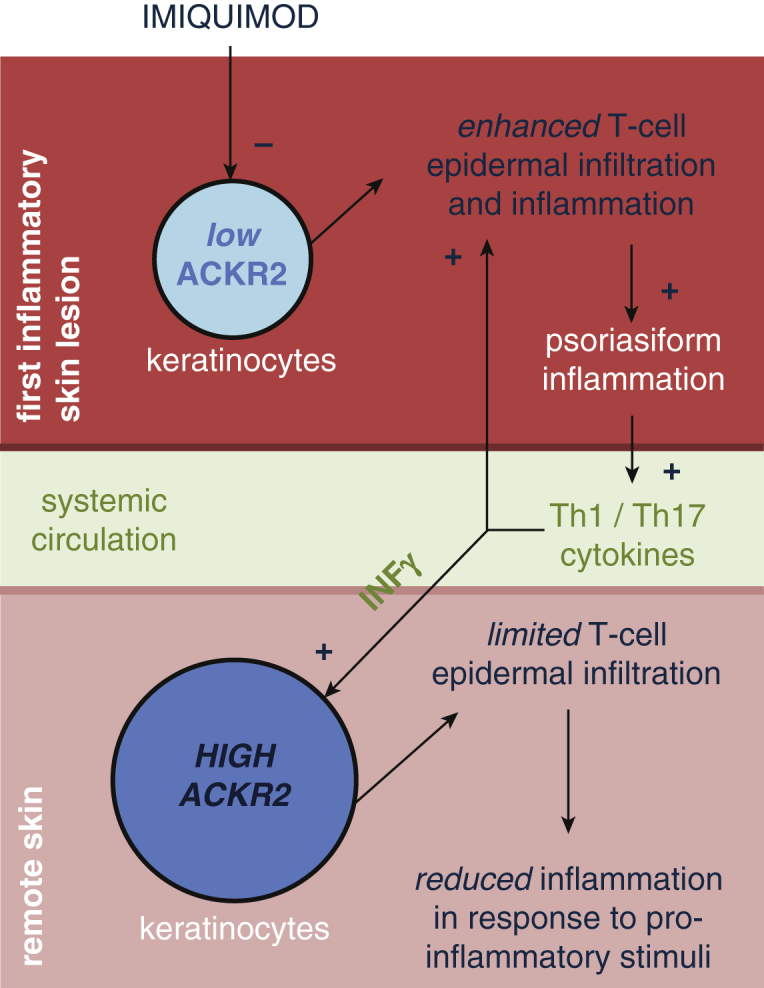
Elucidating the poorly defined mechanisms by which inflammatory lesions are spatially restricted in vivo is of critical importance in understanding skin disease. Chemokines are the principal regulators of leukocyte migration and are essential in the initiation and maintenance of inflammation. The membrane-bound psoriasis-associated atypical chemokine receptor 2 (ACKR2) binds, internalizes and degrades most proinflammatory CC-chemokines. Here we investigate the role of ACKR2 in limiting the spread of cutaneous psoriasiform inflammation to sites that are remote from the primary lesion. Circulating factors capable of regulating ACKR2 function at remote sites were identified and examined using a combination of clinical samples, relevant primary human cell cultures, in vitro migration assays, and the imiquimod-induced model of psoriasiform skin inflammation. Localized inflammation and IFN-γ together up-regulate ACKR2 in remote tissues, protecting them from the spread of inflammation. ACKR2 controls inflammatory T-cell chemotaxis and positioning within the skin, preventing an epidermal influx that is associated with lesion development. Our results have important implications for our understanding of how spatial restriction is imposed on the spread of inflammatory lesions and highlight systemic ACKR2 induction as a therapeutic strategy in the treatment and prevention of psoriasis and potentially a broad range of other immune-mediated diseases.
Copyright © 2016 The Authors. Published by Elsevier Inc. All rights reserved.
Figures





Comment in
-
ACKR2: Nature's Decoy Receptor Lures Unsuspecting Chemokines in Psoriasis.J Invest Dermatol. 2017 Jan;137(1):7-11. doi: 10.1016/j.jid.2016.09.035. J Invest Dermatol. 2017. PMID: 28010760
References
-
- Bachelerie F., Graham G.J., Locati M., Mantovani A., Murphy P.M., Nibbs R. New nomenclature for atypical chemokine receptors. Nat Immunol. 2014;15:207–208. - PubMed
-
- Bazzan E., Saetta M., Turato G., Borroni E.M., Cancellieri C., Baraldo S. Expression of the atypical chemokine receptor D6 in human alveolar macrophages in chronic obstructive pulmonary disease. Chest. 2012;143:98–106. - PubMed
-
- Borroni E.M., Cancellieri C., Vacchini A., Benureau Y., Lagane B., Bachelerie F. Beta-arrestin-dependent activation of the cofilin pathway is required for the scavenging activity of the atypical chemokine receptor D6. Sci Signal. 2013 6 ra30.1–11, S1–3. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
