

Value of Kidney Disease Improving Global Outcomes Urine Output Criteria in Critically Ill Patients: A Secondary Analysis of a Multicenter Prospective Cohort Study
- PMID: 27569230
- PMCID: PMC5009587
- DOI: 10.4103/0366-6999.189059
Value of Kidney Disease Improving Global Outcomes Urine Output Criteria in Critically Ill Patients: A Secondary Analysis of a Multicenter Prospective Cohort Study
Abstract
Background: Urine output (UO) is an essential criterion of the Kidney Disease Improving Global Outcomes (KDIGO) definition and classification system for acute kidney injury (AKI), of which the diagnostic value has not been extensively studied. We aimed to determine whether AKI based on KDIGO UO criteria (KDIGOUO) could improve the diagnostic and prognostic accuracy, compared with KDIGO serum creatinine criteria (KDIGOSCr).
Methods: We conducted a secondary analysis of the database of a previous study conducted by China Critical Care Clinical Trial Group (CCCCTG), which was a 2-month prospective cohort study (July 1, 2009 to August 31, 2009) involving 3063 patients in 22 tertiary Intensive Care Units in Mainland of China. AKI was diagnosed and classified separately based on KDIGOUOand KDIGOSCr. Hospital mortality of patients with more severe AKI classification based on KDIGOUOwas compared with other patients by univariate and multivariate regression analyses.
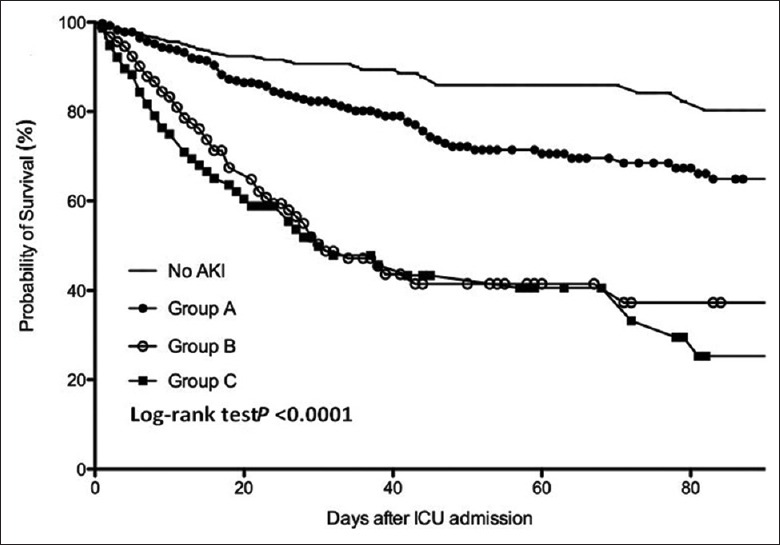
Results: The prevalence of AKI increased from 52.4% based on KDIGOSCrto 55.4% based on KDIGOSCrcombined with KDIGOUO. KDIGOUOalso resulted in an upgrade of AKI classification in 7.3% of patients, representing those with more severe AKI classification based on KDIGOUO. Compared with non-AKI patients or those with maximum AKI classification by KDIGOSCr, those with maximum AKI classification by KDIGOUOhad a significantly higher hospital mortality of 58.4% (odds ratio [OR]: 7.580, 95% confidence interval [CI]: 4.141-13.873, P< 0.001). In a multivariate logistic regression analysis, AKI based on KDIGOUO (OR: 2.891, 95% CI: 1.964-4.254, P< 0.001), but not based on KDIGOSCr (OR: 1.322, 95% CI: 0.902-1.939, P = 0.152), was an independent risk factor for hospital mortality.
Conclusion: UO was a criterion with additional value beyond creatinine criterion for AKI diagnosis and classification, which can help identify a group of patients with high risk of death.
Figures

Similar articles
-
[Stratified outcomes of "Kidney Disease: Improving Global Outcomes" serum creatinine criteria in critical ill patients: a secondary analysis of a multicenter prospective study].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020 Mar;32(3):313-318. doi: 10.3760/cma.j.cn121430-20200218-00192. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020. PMID: 32385995 Chinese.
-
Acute Kidney Injury Classified by Serum Creatinine and Urine Output in Critically Ill Cancer Patients.Biomed Res Int. 2016;2016:6805169. doi: 10.1155/2016/6805169. Epub 2016 Oct 10. Biomed Res Int. 2016. PMID: 27803928 Free PMC article.
-
Optimum methodology for estimating baseline serum creatinine for the acute kidney injury classification.Nephrology (Carlton). 2015 Dec;20(12):881-6. doi: 10.1111/nep.12525. Nephrology (Carlton). 2015. PMID: 26032233
-
Incidence, timing and outcome of AKI in critically ill patients varies with the definition used and the addition of urine output criteria.BMC Nephrol. 2017 Feb 20;18(1):70. doi: 10.1186/s12882-017-0487-8. BMC Nephrol. 2017. PMID: 28219327 Free PMC article. Review.
-
Acute Kidney Injury: Diagnosis and Classification in Adults and Children.Contrib Nephrol. 2018;193:1-12. doi: 10.1159/000484956. Epub 2018 Jan 23. Contrib Nephrol. 2018. PMID: 29393148 Review.
Cited by
-
Identification of an optimal threshold to define oliguria in critically ill patients: an observational study.Crit Care. 2023 May 30;27(1):207. doi: 10.1186/s13054-023-04505-7. Crit Care. 2023. PMID: 37254158 Free PMC article.
-
Urine output is an early and strong predictor of acute kidney injury and associated mortality: a systematic literature review of 50 clinical studies.Ann Intensive Care. 2024 Jul 9;14(1):110. doi: 10.1186/s13613-024-01342-x. Ann Intensive Care. 2024. PMID: 38980557 Free PMC article. Review.
-
Pathogenesis and Management of Acute Kidney Injury in Patients with Nephrotic Syndrome Due to Primary Glomerulopathies.Medicina (Kaunas). 2019 Jul 11;55(7):365. doi: 10.3390/medicina55070365. Medicina (Kaunas). 2019. PMID: 31336742 Free PMC article. Review.
-
Association of Oliguria With Acute Kidney Injury Diagnosis, Severity Assessment, and Mortality Among Patients With Critical Illness.JAMA Netw Open. 2021 Nov 1;4(11):e2133094. doi: 10.1001/jamanetworkopen.2021.33094. JAMA Netw Open. 2021. PMID: 34735011 Free PMC article.
-
The Role of Oliguria and the Absence of Fluid Administration and Balance Information in Illness Severity Scores.Korean J Crit Care Med. 2017 May;32(2):106-123. doi: 10.4266/kjccm.2017.00192. Epub 2017 May 31. Korean J Crit Care Med. 2017. PMID: 31723625 Free PMC article. Review.
References
-
- Chertow GM, Levy EM, Hammermeister KE, Grover F, Daley J. Independent association between acute renal failure and mortality following cardiac surgery. Am J Med. 1998;104:343–8. doi: 10.1016/S0002-9343(98)00058-8. - PubMed
-
- de Mendonça A, Vincent JL, Suter PM, Moreno R, Dearden NM, Antonelli M, et al. Acute renal failure in the ICU: Risk factors and outcome evaluated by the SOFA score. Intensive Care Med. 2000;26:915–21. doi: 10.1007/s001340051281. - PubMed
-
- Nash K, Hafeez A, Hou S. Hospital-acquired renal insufficiency. Am J Kidney Dis. 2002;39:930–6. doi: 10.1053/ajkd.2002.32766. - PubMed
-
- Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, et al. Acute renal failure in critically ill patients: A multinational, multicenter study. JAMA. 2005;294:813–8. doi: 10.1001/jama. 294.7.813. - PubMed
-
- Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P. Acute renal failure – Definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2004;8:R204–12. doi: 10.1186/cc2872. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
