

Medication use and the risk of motor vehicle collisions among licensed drivers: A systematic review
- PMID: 27569655
- PMCID: PMC5045819
- DOI: 10.1016/j.aap.2016.08.001
Medication use and the risk of motor vehicle collisions among licensed drivers: A systematic review
Abstract
Objectives: Driving under the influence of prescription and over-the-counter medication is a growing public health concern. A systematic review of the literature was performed to investigate which specific medications were associated with increased risk of motor vehicle collision (MVC).
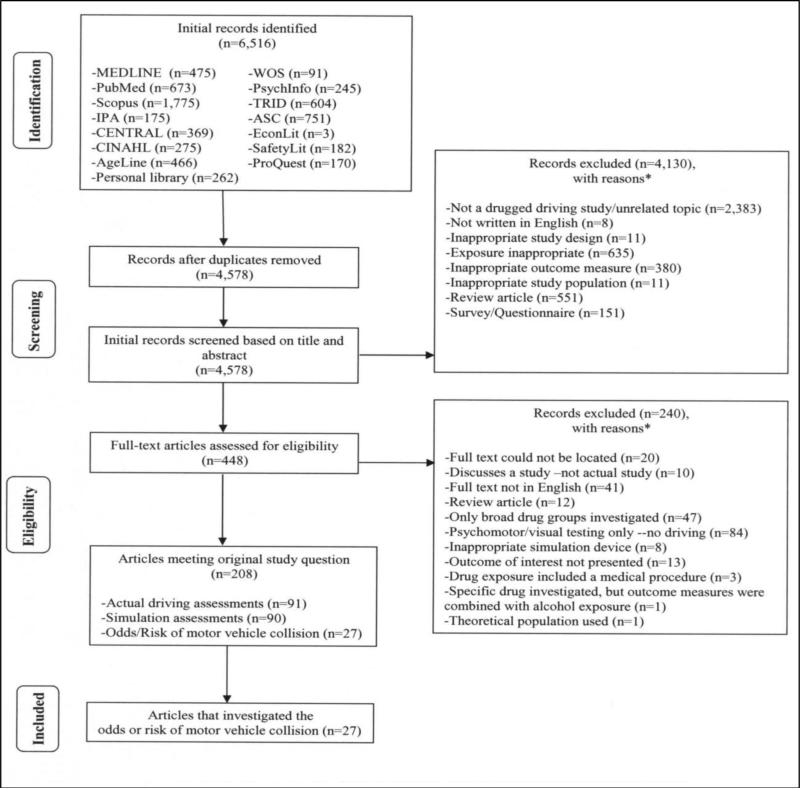
Methods: The a priori inclusion criteria were: (1) studies published from English-language sources on or after January 1, 1960, (2) licensed drivers 15 years of age and older, (3) peer-reviewed publications, master's theses, doctoral dissertations, and conference papers, (4) studies limited to randomized control trials, cohort studies, case-control studies, or case-control type studies (5) outcome measure reported for at least one specific medication, (6) outcome measure reported as the odds or risk of a motor vehicle collision. Fourteen databases were examined along with hand-searching. Independent, dual selection of studies and data abstraction was performed.
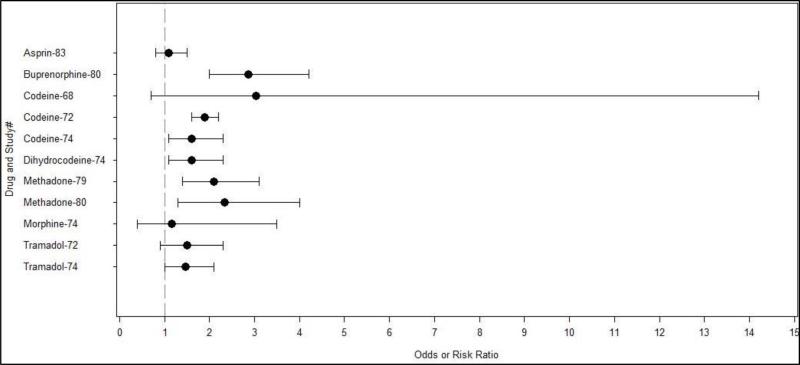
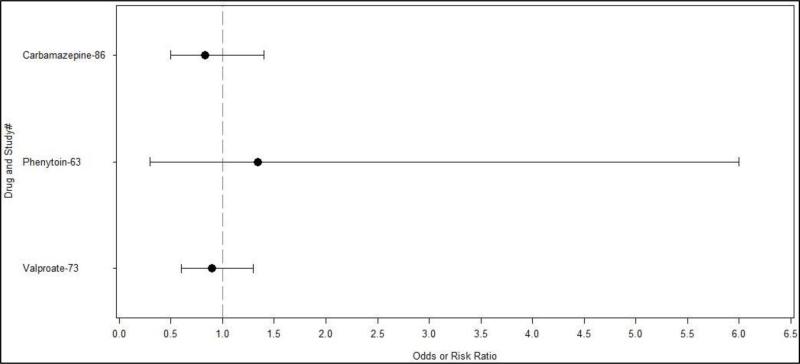
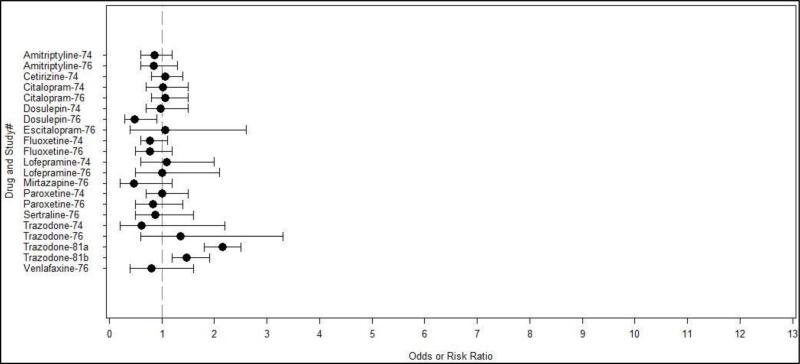
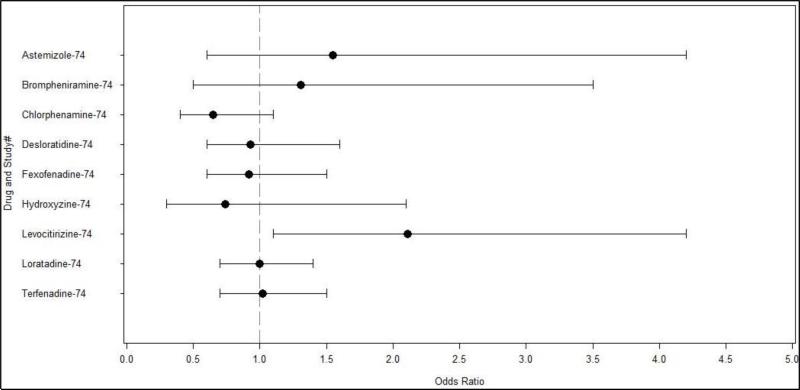
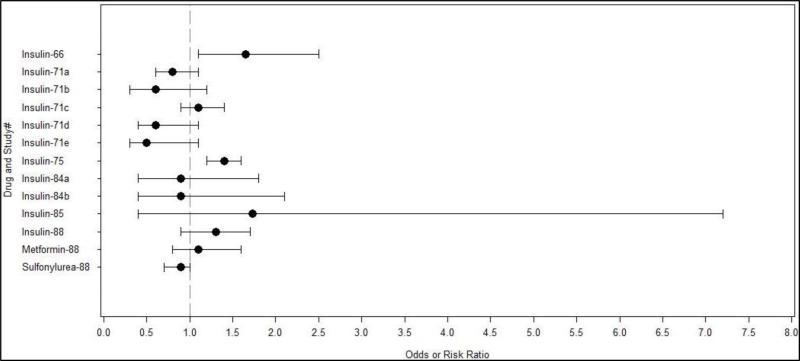
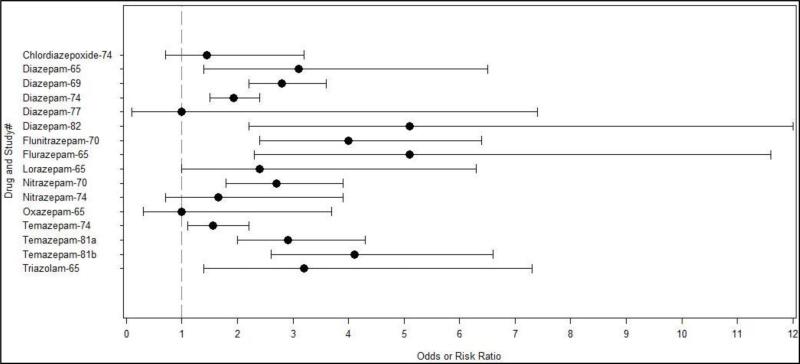
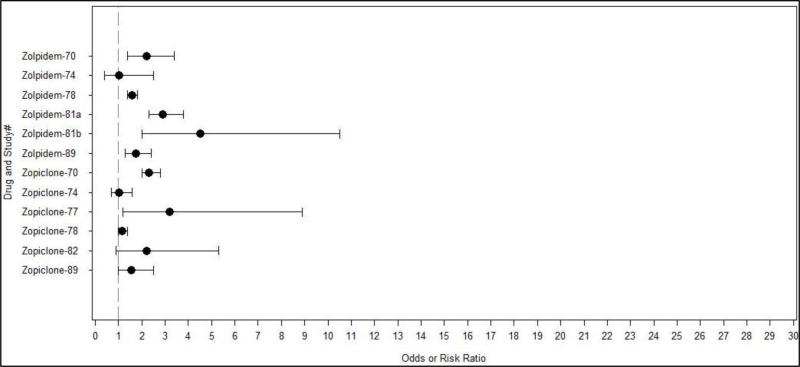
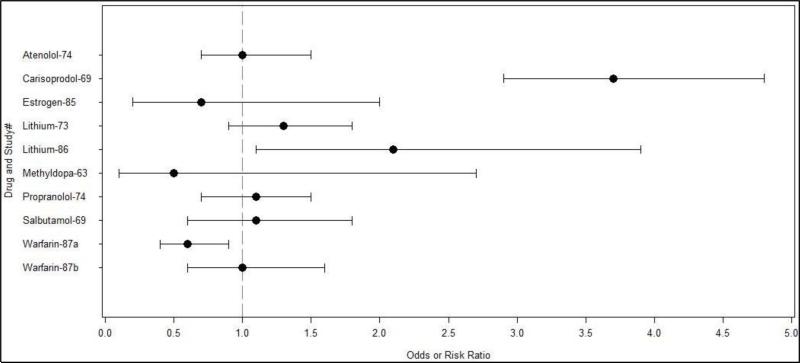
Results: Fifty-three medications were investigated by 27 studies included in the review. Fifteen (28.3%) were associated with an increased risk of MVC. These included Buprenorphine, Codeine, Dihydrocodeine, Methadone, Tramadol, Levocitirizine, Diazepam, Flunitrazepam, Flurazepam, Lorazepam, Temazepam, Triazolam, Carisoprodol, Zolpidem, and Zopiclone.
Conclusions: Several medications were associated with an increased risk of MVC and decreased driving ability. The associations between specific medication use and the increased risk of MVC and/or affected driving ability are complex. Future research opportunities are plentiful and worthy of such investigation.
Keywords: Ability; Driving; Drugs; Prescription; Review.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Figures
References
-
- Sise RG, Calvo RY, Spain DA, Weiser TG, Staudenmayer KL. The epidemiology of trauma-related mortality in the United States from 2002 to 2010. The journal of trauma and acute care surgery. 2014 Apr;76(4):913–919. discussion 920. - PubMed
-
- Oster CV, Strong J. Analyzing road safety in the United States. Res. Transp. Econ. 2013;43:98–111.
-
- Morland J. Driving under the influence of non-alcohol drugs. Forensic Sci.Rev. 2000;12:80–105. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
