

SIAH and EGFR, Two RAS Pathway Biomarkers, are Highly Prognostic in Locally Advanced and Metastatic Breast Cancer
- PMID: 27569656
- PMCID: PMC5049993
- DOI: 10.1016/j.ebiom.2016.08.014
SIAH and EGFR, Two RAS Pathway Biomarkers, are Highly Prognostic in Locally Advanced and Metastatic Breast Cancer
Abstract
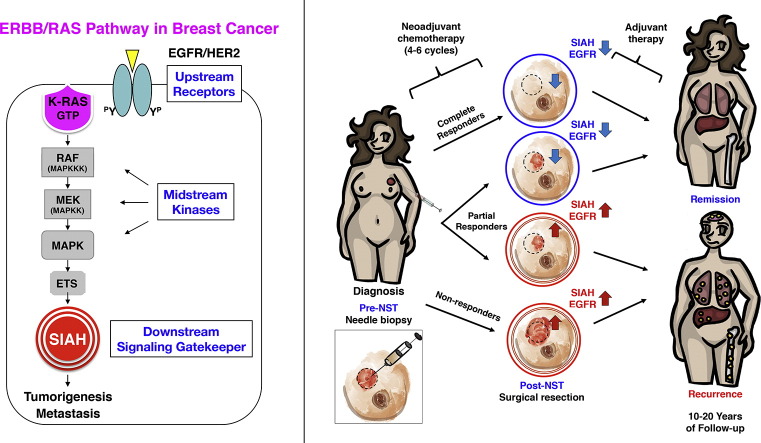
Background: Metastatic breast cancer exhibits diverse and rapidly evolving intra- and inter-tumor heterogeneity. Patients with similar clinical presentations often display distinct tumor responses to standard of care (SOC) therapies. Genome landscape studies indicate that EGFR/HER2/RAS "pathway" activation is highly prevalent in malignant breast cancers. The identification of therapy-responsive and prognostic biomarkers is paramount important to stratify patients and guide therapies in clinical oncology and personalized medicine.
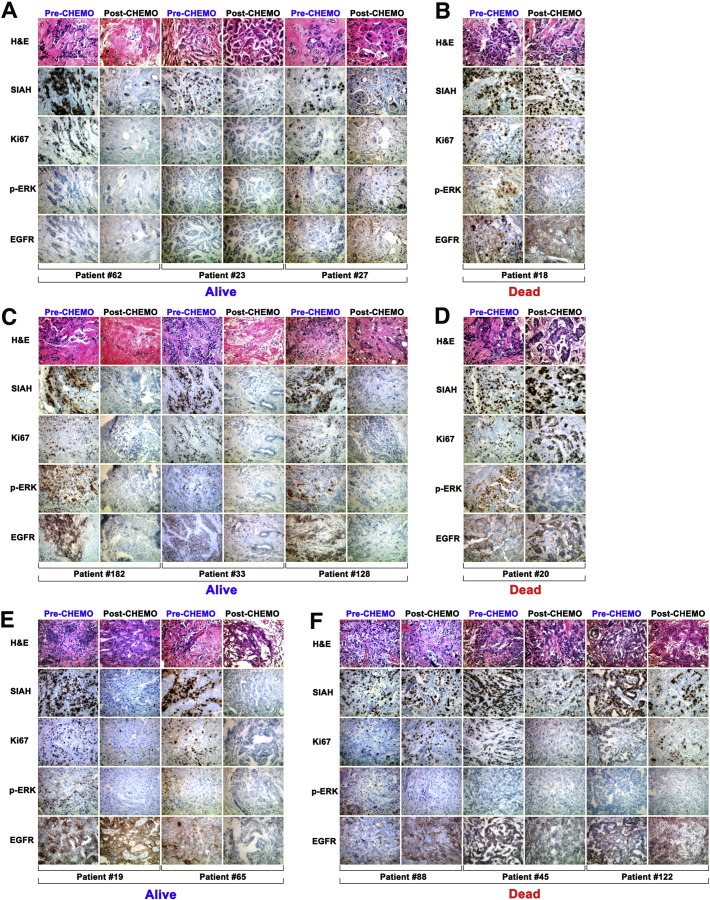
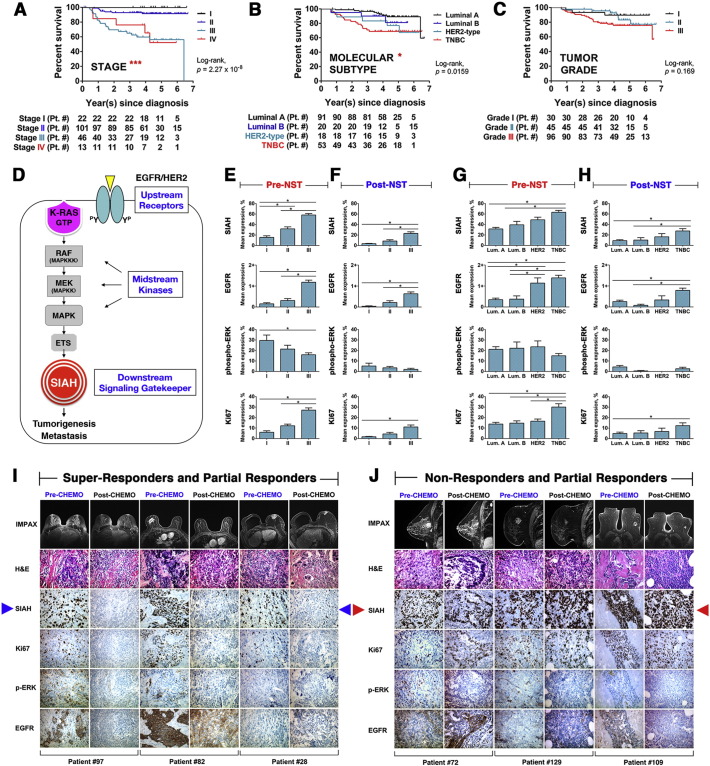
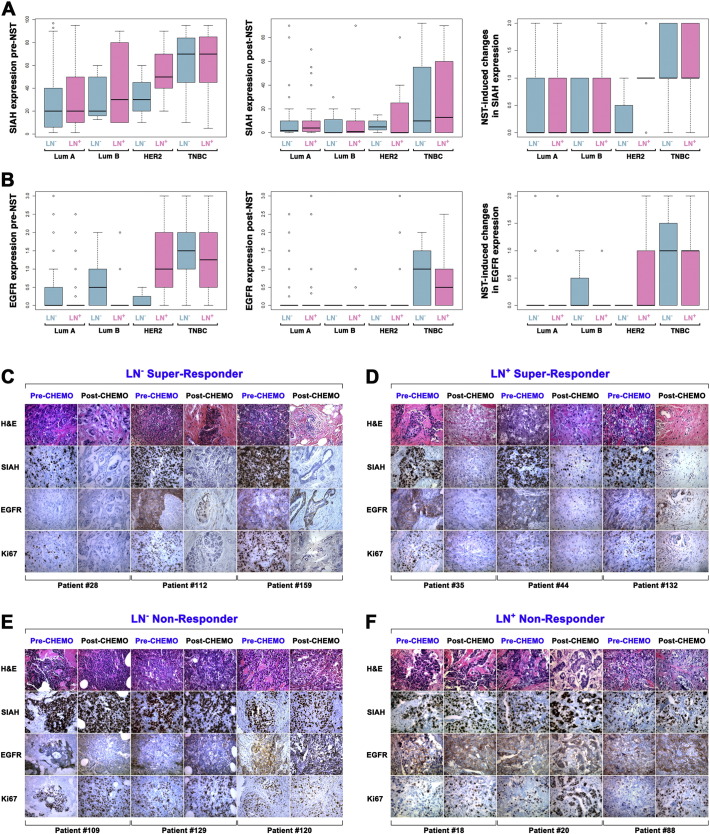
Methods: In this study, we analyzed matched pairs of tumor specimens collected from 182 patients who received neoadjuvant systemic therapies (NST). Statistical analyses were conducted to determine whether EGFR/HER2/RAS pathway biomarkers and clinicopathological predictors, alone and in combination, are prognostic in breast cancer.
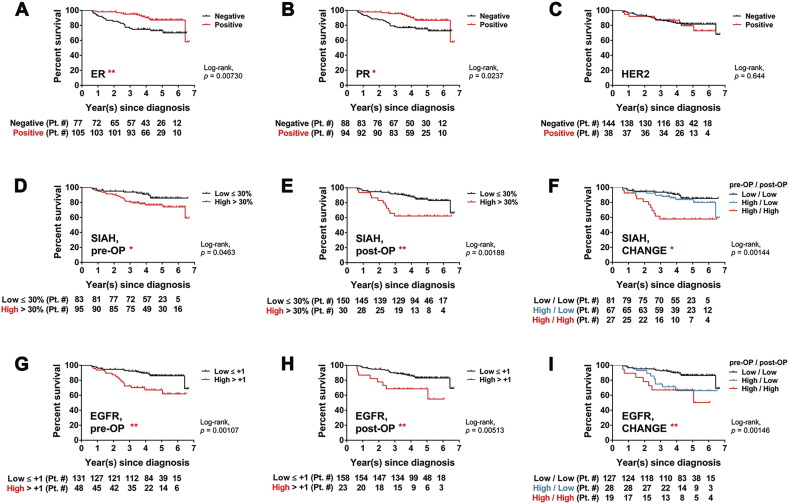
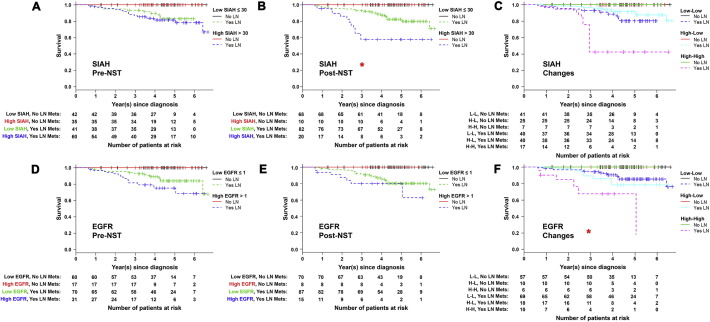
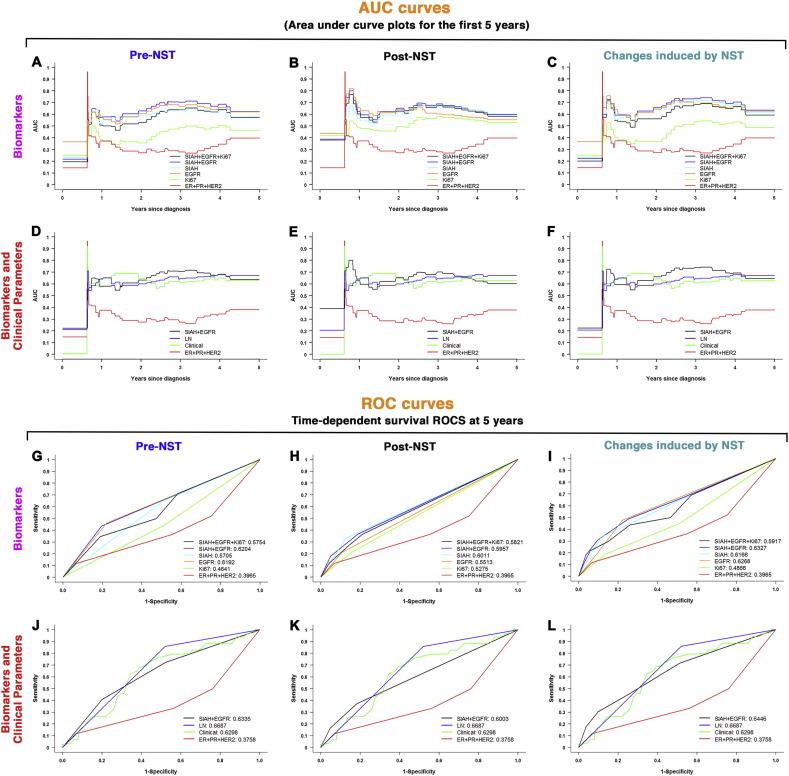
Findings: SIAH and EGFR outperform ER, PR, HER2 and Ki67 as two logical, sensitive and prognostic biomarkers in metastatic breast cancer. We found that increased SIAH and EGFR expression correlated with advanced pathological stage and aggressive molecular subtypes. Both SIAH expression post-NST and NST-induced changes in EGFR expression in invasive mammary tumors are associated with tumor regression and increased survival, whereas ER, PR, and HER2 were not. These results suggest that SIAH and EGFR are two prognostic biomarkers in breast cancer with lymph node metastases.
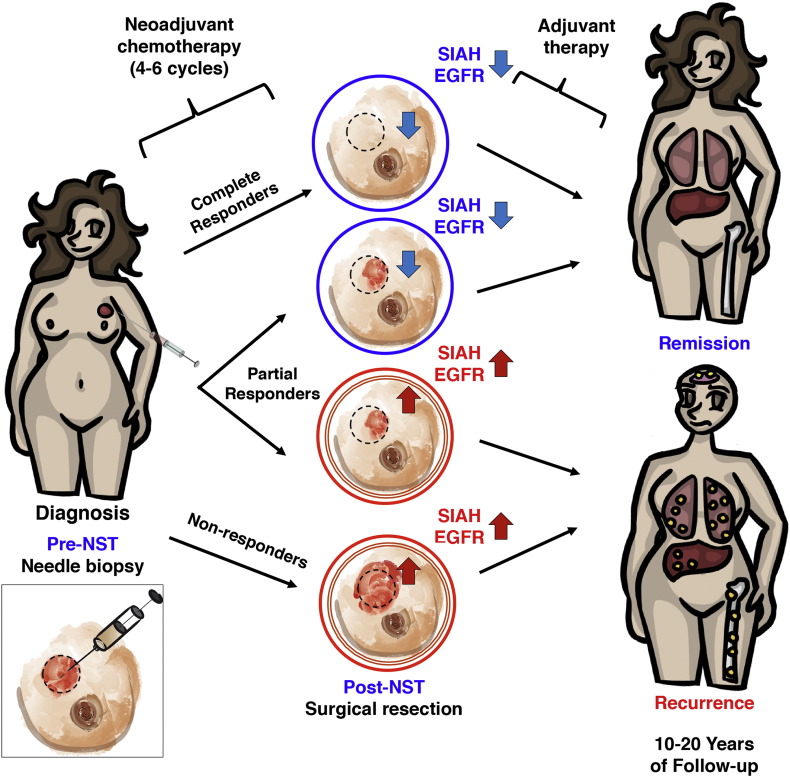
Interpretation: The discovery of incorporating tumor heterogeneity-independent and growth-sensitive RAS pathway biomarkers, SIAH and EGFR, whose altered expression can be used to estimate therapeutic efficacy, detect emergence of resistant clones, forecast tumor regression, differentiate among partial responders, and predict patient survival in the neoadjuvant setting, has a clear clinical implication in personalizing breast cancer therapy.
Funding: This work was supported by the Dorothy G. Hoefer Foundation for Breast Cancer Research (A.H. Tang); Center for Innovative Technology (CIT)-Commonwealth Research Commercialization Fund (CRCF) (MF14S-009-LS to A.H. Tang), and National Cancer Institute (CA140550 to A.H. Tang).
Keywords: And prognostic biomarkers; Clinicopathological predictors; Locally advanced and metastatic breast cancer; Needle biopsies; Neoadjuvant systemic therapies; SIAH E3 ligase; The RAS pathway activation in breast cancer.
Copyright © 2016 Forschungsgesellschaft für Arbeitsphysiologie und Arbeitschutz e.V. Published by Elsevier B.V. All rights reserved.
Figures
References
-
- Albain K.S., Barlow W.E., Shak S., Hortobagyi G.N., Livingston R.B., Yeh I.T., Ravdin P., Bugarini R., Baehner F.L., Davidson N.E. Prognostic and predictive value of the 21-gene recurrence score assay in postmenopausal women with node-positive, oestrogen-receptor-positive breast cancer on chemotherapy: a retrospective analysis of a randomised trial. Lancet Oncol. 2010;11:55–65. - PMC - PubMed
-
- Arteaga C.L., Sliwkowski M.X., Osborne C.K., Perez E.A., Puglisi F., Gianni L. Treatment of HER2-positive breast cancer: current status and future perspectives. Nat. Rev. Clin. Oncol. 2012;9:16–32. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
