

Intracerebral Hemorrhage Outcomes in Patients with Systemic Cancer
- PMID: 27569708
- PMCID: PMC5344037
- DOI: 10.1016/j.jstrokecerebrovasdis.2016.08.006
Intracerebral Hemorrhage Outcomes in Patients with Systemic Cancer
Abstract
Background: Single-center studies suggest that patients with cancer have similar outcomes after intracerebral hemorrhage (ICH) compared to patients without cancer. However, these studies were limited by small sample sizes and high rates of intratumoral hemorrhage. Our hypothesis was that systemic cancer patients without brain involvement fare worse after ICH than patients without cancer.
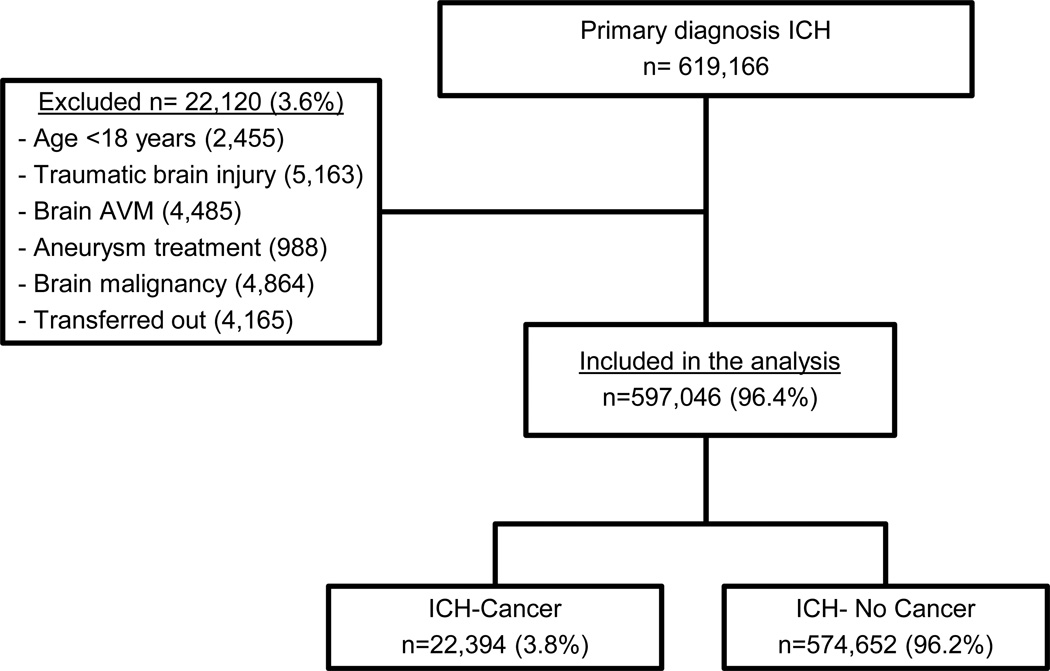
Methods: We identified all patients diagnosed with spontaneous ICH from 2002 to 2011 in the Nationwide Inpatient Sample. Our predictor variable was systemic cancer. Our primary outcome was discharge disposition, dichotomized into favorable discharge (home/self-care or rehabilitation) or unfavorable discharge (nursing facility, hospice, or death). We used logistic regression to compare outcomes and performed secondary analyses by cancer subtype (i.e., nonmetastatic solid tumors, nonmetastatic hematologic tumors, and metastatic solid or hematologic tumors).
Results: Among 597,046 identified ICH patients, 22,394 (3.8%) had systemic cancer. Stroke risk factors such as hypertension and diabetes were more common in patients without cancer, whereas anticoagulant use and higher Charlson comorbidity scores were more common among cancer patients. In multivariate logistic regression analysis adjusted for demographics, comorbidities, and hospital-level characteristics, patients with cancer had higher odds of death (OR 1.62, 95% CI 1.56-1.69) and lower odds of favorable discharge (OR .59, 95% CI .56-.63) than patients without cancer. Among cancer groups, patients with nonmetastatic hematologic tumors and those with metastatic disease fared the worst.
Conclusions: Patients with systemic cancer have higher mortality and less favorable discharge outcomes after ICH than patients without cancer. Cancer subtype may influence outcomes after ICH.
Keywords: Intracerebral hemorrhage; cancer; clinical outcomes; malignancy.
Copyright © 2016 National Stroke Association. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have no conflict of interests to report.
Figures
Similar articles
-
Designated Stroke Center Status and Hospital Characteristics as Predictors of In-Hospital Mortality among Hemorrhagic Stroke Patients in New York, 2008-2012.Cerebrovasc Dis. 2017;43(1-2):43-53. doi: 10.1159/000451033. Epub 2016 Nov 15. Cerebrovasc Dis. 2017. PMID: 27842319
-
Outcomes after intracerebral hemorrhage from arteriovenous malformations.Neurology. 2017 May 16;88(20):1882-1888. doi: 10.1212/WNL.0000000000003935. Epub 2017 Apr 19. Neurology. 2017. PMID: 28424275 Free PMC article.
-
Presence of Concomitant Systemic Cancer is Not Associated with Worse Functional Long-Term Outcome in Patients with Intracerebral Hemorrhage.Cerebrovasc Dis. 2017;44(3-4):186-194. doi: 10.1159/000479075. Epub 2017 Aug 3. Cerebrovasc Dis. 2017. PMID: 28768267
-
The role of age in intracerebral hemorrhages.J Clin Neurosci. 2015 Dec;22(12):1867-70. doi: 10.1016/j.jocn.2015.04.020. Epub 2015 Sep 12. J Clin Neurosci. 2015. PMID: 26375325 Review.
-
Nontraumatic intracerebral haemorrhage in young adults.Nat Rev Neurol. 2018 Apr;14(4):237-250. doi: 10.1038/nrneurol.2018.17. Epub 2018 Mar 9. Nat Rev Neurol. 2018. PMID: 29521335 Review.
Cited by
-
Patients with Invasive Tumors and eNOS Gene Polymorphisms with Subarachnoid Hemorrhage Tend to Have Poorer Prognosis.Asian J Neurosurg. 2022 Aug 24;17(2):199-208. doi: 10.1055/s-0042-1750784. eCollection 2022 Jun. Asian J Neurosurg. 2022. PMID: 36120623 Free PMC article.
-
Cancer and stroke: commonly encountered by clinicians, but little evidence to guide clinical approach.Ther Adv Neurol Disord. 2022 Jun 28;15:17562864221106362. doi: 10.1177/17562864221106362. eCollection 2022. Ther Adv Neurol Disord. 2022. PMID: 35785404 Free PMC article. Review.
-
Cost-utility analysis of apixaban compared with usual care for primary thromboprophylaxis in ambulatory patients with cancer.CMAJ. 2021 Oct 12;193(40):E1551-E1560. doi: 10.1503/cmaj.210523. CMAJ. 2021. PMID: 35040802 Free PMC article.
-
Cerebrovascular and Peripheral Vascular Complications in Cancer Patients.Curr Neurol Neurosci Rep. 2025 Jul 1;25(1):46. doi: 10.1007/s11910-025-01434-6. Curr Neurol Neurosci Rep. 2025. PMID: 40591095 Review.
-
Clinical Characteristics and Risk Factors of Cerebral Hemorrhage in Patients with Occult Malignant Tumors.Neuropsychiatr Dis Treat. 2021 Aug 19;17:2729-2738. doi: 10.2147/NDT.S321571. eCollection 2021. Neuropsychiatr Dis Treat. 2021. PMID: 34434047 Free PMC article.
References
-
- McCormick WF, Rosenfield DB. Massive brain hemorrhage: a review of 144 cases and an examination of their causes. Stroke. 1973;4(6):946–954. - PubMed
-
- Schrader B, Barth H, Lang EW, Buhl R, Hugo HH, Biederer J, et al. Spontaneous intracranial haematomas caused by neoplasms. Acta neurochirurgica. 2000;142(9):979–985. - PubMed
-
- Velander AJ, DeAngelis LM, Navi BB. Intracranial hemorrhage in patients with cancer. Curr Atheroscler Rep. 2012;14(4):373–381. - PubMed
-
- Licata B, Turazzi S. Bleeding cerebral neoplasms with symptomatic hematoma. J Neurosurg Sci. 2003;47(4):201–210. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
