

In Children With Nonalcoholic Fatty Liver Disease, Cysteamine Bitartrate Delayed Release Improves Liver Enzymes but Does Not Reduce Disease Activity Scores
- PMID: 27569726
- PMCID: PMC5124386
- DOI: 10.1053/j.gastro.2016.08.027
In Children With Nonalcoholic Fatty Liver Disease, Cysteamine Bitartrate Delayed Release Improves Liver Enzymes but Does Not Reduce Disease Activity Scores
Abstract
Background & aims: No treatment for nonalcoholic fatty liver disease (NAFLD) has been approved by regulatory agencies. We performed a randomized controlled trial to determine whether 52 weeks of cysteamine bitartrate delayed release (CBDR) reduces the severity of liver disease in children with NAFLD.
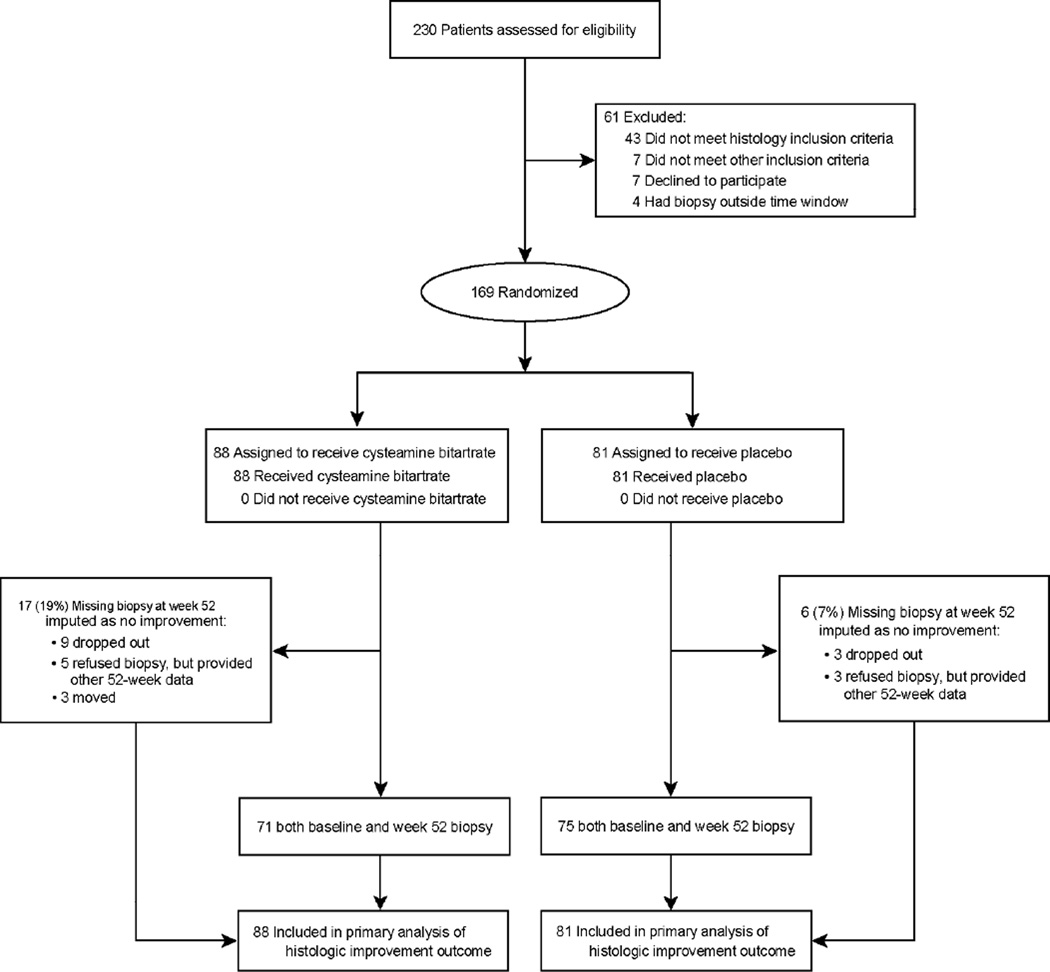
Methods: We performed a double-masked trial of 169 children with NAFLD activity scores of 4 or higher at 10 centers. From June 2012 to January 2014, the patients were assigned randomly to receive CBDR or placebo twice daily (300 mg for patients weighing ≤65 kg, 375 mg for patients weighing >65 to 80 kg, and 450 mg for patients weighing >80 kg) for 52 weeks. The primary outcome from the intention-to-treat analysis was improvement in liver histology over 52 weeks, defined as a decrease in the NAFLD activity score of 2 points or more without worsening fibrosis; patients without biopsy specimens from week 52 (17 in the CBDR group and 6 in the placebo group) were considered nonresponders. We calculated the relative risks (RR) of improvement using a stratified Cochran-Mantel-Haenszel analysis.
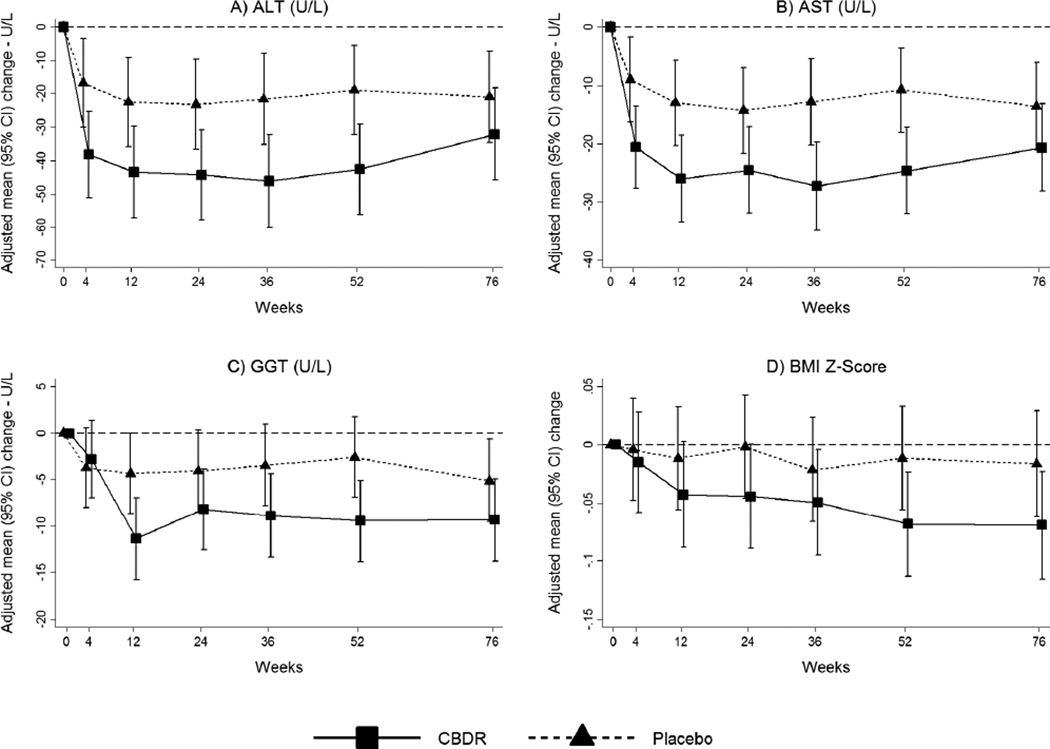
Results: There was no significant difference between groups in the primary outcome (28% of children in the CBDR group vs 22% in the placebo group; RR, 1.3; 95% confidence interval [CI], 0.8-2.1; P = .34). However, children receiving CBDR had significant changes in prespecified secondary outcomes: reduced mean levels of alanine aminotransferase (reduction, 53 ± 88 U/L vs 8 ± 77 U/L in the placebo group; P = .02) and aspartate aminotransferase (reduction, 31 ± 52 vs 4 ± 36 U/L in the placebo group; P = .008), and a larger proportion had reduced lobular inflammation (36% in the CBDR group vs 21% in the placebo group; RR, 1.8; 95% CI, 1.1-2.9; P = .03). In a post hoc analysis of children weighing 65 kg or less, those taking CBDR had a 4-fold better chance of histologic improvement (observed in 50% of children in the CBDR group vs 13% in the placebo group; RR, 4.0; 95% CI, 1.3-12.3; P = .005).
Conclusions: In a randomized trial, we found that 1 year of CBDR did not reduce overall histologic markers of NAFLD compared with placebo in children. Children receiving CBDR, however, had significant reductions in serum aminotransferase levels and lobular inflammation. ClinicalTrials.gov no: NCT01529268.
Keywords: ALT; AST; Obesity; Pediatrics.
Copyright © 2016 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Schwimmer JB, Deutsch R, Kahen T, et al. Prevalence of fatty liver in children and adolescents. Pediatrics. 2006;118:1388–1393. - PubMed
-
- Schwimmer JB, Behling C, Newbury R, et al. Histopathology of pediatric nonalcoholic fatty liver disease. Hepatology. 2005;42:641–649. - PubMed
-
- Lindback SM, Gabbert C, Johnson BL, et al. Pediatric nonalcoholic fatty liver disease: a comprehensive review. Adv Pediatr. 2010;57:85–140. - PubMed
-
- Jung DH, Shim JY, Lee HR, et al. Relationship between non-alcoholic fatty liver disease and pulmonary function. Intern Med J. 2012;42:541–546. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U01 DK061737/DK/NIDDK NIH HHS/United States
- U01 DK061713/DK/NIDDK NIH HHS/United States
- U01 DK061732/DK/NIDDK NIH HHS/United States
- UL1 TR000150/TR/NCATS NIH HHS/United States
- U01 DK061731/DK/NIDDK NIH HHS/United States
- U01 DK061718/DK/NIDDK NIH HHS/United States
- UL1 TR001442/TR/NCATS NIH HHS/United States
- P30 DK089502/DK/NIDDK NIH HHS/United States
- P30 DK078392/DK/NIDDK NIH HHS/United States
- UL1 TR000006/TR/NCATS NIH HHS/United States
- UL1 TR001108/TR/NCATS NIH HHS/United States
- UL1 TR001422/TR/NCATS NIH HHS/United States
- U01 DK061730/DK/NIDDK NIH HHS/United States
- U01 DK061728/DK/NIDDK NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- U01 DK061738/DK/NIDDK NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- UL1 TR000448/TR/NCATS NIH HHS/United States
- U01 DK061734/DK/NIDDK NIH HHS/United States
- UL1 TR001425/TR/NCATS NIH HHS/United States
- P30 DK048522/DK/NIDDK NIH HHS/United States
- UL1 TR002319/TR/NCATS NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- UL1 TR000077/TR/NCATS NIH HHS/United States
- UL1 TR000423/TR/NCATS NIH HHS/United States
- UL1 TR000100/TR/NCATS NIH HHS/United States
- UL1 TR000004/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
