

Risk factor for ischemic-type biliary lesion after ABO-incompatible living donor liver transplantation
- PMID: 27570428
- PMCID: PMC4974590
- DOI: 10.3748/wjg.v22.i30.6925
Risk factor for ischemic-type biliary lesion after ABO-incompatible living donor liver transplantation
Abstract
Aim: To evaluate the risk factors for ischemic-type biliary lesion (ITBL) after ABO-incompatible (ABO-I) adult living donor liver transplantation (ALDLT).
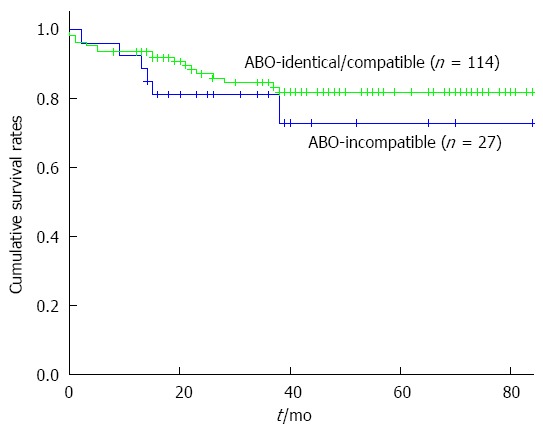
Methods: Among 141 ALDLTs performed in our hospital between 2008 and 2014, 27 (19%) were ABO-I ALDLT and 114 were ABO-identical/compatible ALDLT. In this study, we extensively analyzed the clinico-pathological data of the 27 ABO-I recipients to determine the risk factors for ITBL after ABO-I ALDLT. All ABO-I ALDLT recipients underwent an identical B-cell depletion protocol with preoperative rituximab, plasma exchange (PE), and operative splenectomy. The median follow-up period after transplantation was 26 mo. The clinical outcomes of the 27 ABO-I ALDLT recipients were compared with those of 114 ABO-identical/compatible ALDLT recipients.
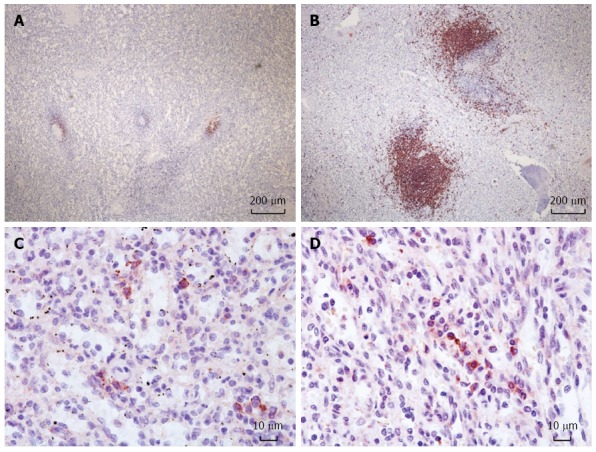
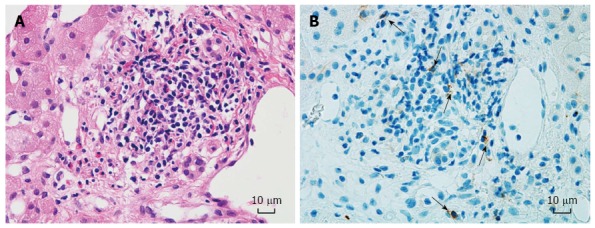
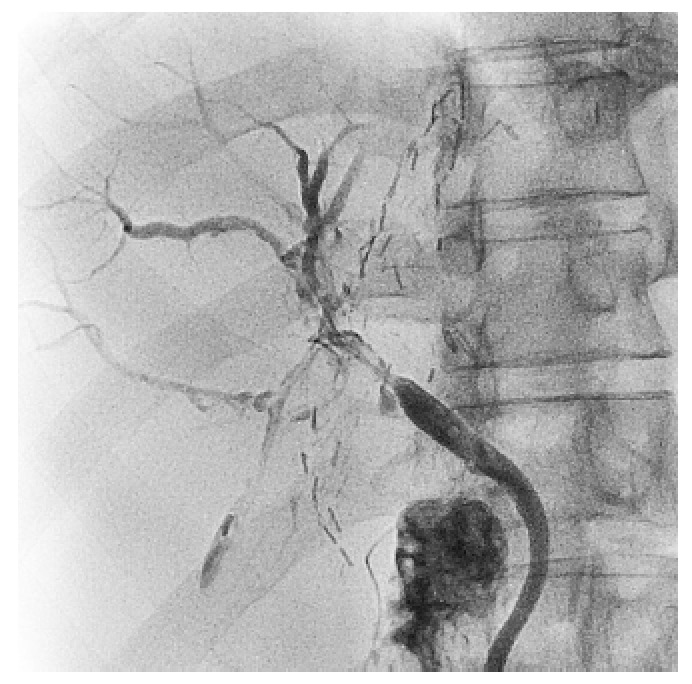
Results: ITBL occurred in four recipients (14.8%) between 45 and 112 d after ABO-I ALDLT. The overall survival rates were not different between ABO-I ALDLT and ABO-identical/compatible ALDLT (P = 0.303). Among the ABO-I ALDLT recipients, there was no difference between patients with ITBL and those without ITBL in terms of B-cell and T-cell count, serum isoagglutinin titers, number of PEs, operative time and transfusion, use of graft infusion therapy, or number of remnant B-cell follicles and plasma cells in the spleen. However, the perioperative NK cell counts in the blood of patients with ITBL were significantly higher than those in the patients without ITBL (P < 0.05). Preoperative NK cell count > 150/μL and postoperative NK cell count > 120/μL were associated with greater relative risks (RR) for development of ITBL (RR = 20 and 14.3, respectively, P < 0.05).
Conclusion: High NK cell counts in a transplant recipient's blood are associated with ITBL after ABO-I ALDLT. Further research is needed to elucidate the molecular mechanism of NK cell involvement in the development of ITBL.
Keywords: ABO-incompatibility; Ischemic-type biliary lesion; Liver transplantation; Natural killer cell.
Figures
References
-
- Egawa H, Teramukai S, Haga H, Tanabe M, Fukushima M, Shimazu M. Present status of ABO-incompatible living donor liver transplantation in Japan. Hepatology. 2008;47:143–152. - PubMed
-
- Ikegami T, Taketomi A, Soejima Y, Yoshizumi T, Uchiyama H, Harada N, Iguchi T, Hashimoto N, Maehara Y. Rituximab, IVIG, and plasma exchange without graft local infusion treatment: a new protocol in ABO incompatible living donor liver transplantation. Transplantation. 2009;88:303–307. - PubMed
-
- Raut V, Mori A, Kaido T, Ogura Y, Taku I, Nagai K, Sasaki N, Endo K, Hata T, Yagi S, et al. Splenectomy does not offer immunological benefits in ABO-incompatible liver transplantation with a preoperative rituximab. Transplantation. 2012;93:99–105. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
