

Pulsed low-dose RANKL as a potential therapeutic for postmenopausal osteoporosis
- PMID: 27570837
- PMCID: PMC4996279
- DOI: 10.1172/jci.insight.88839
Pulsed low-dose RANKL as a potential therapeutic for postmenopausal osteoporosis
Abstract
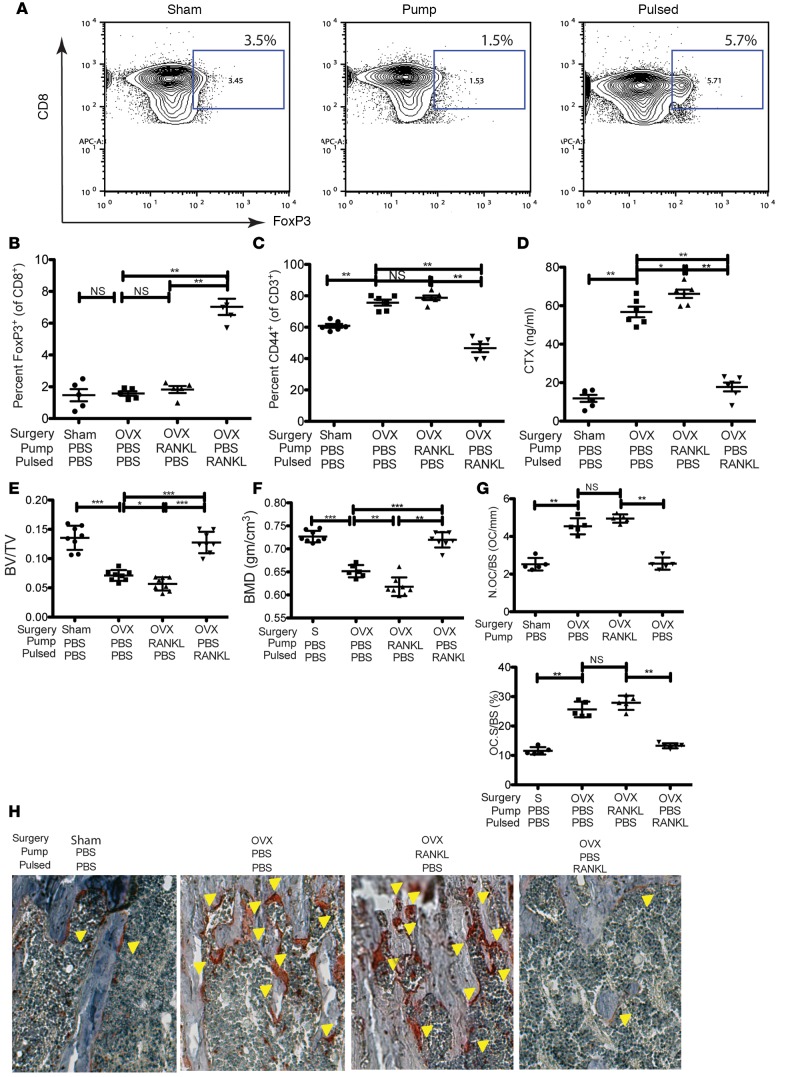
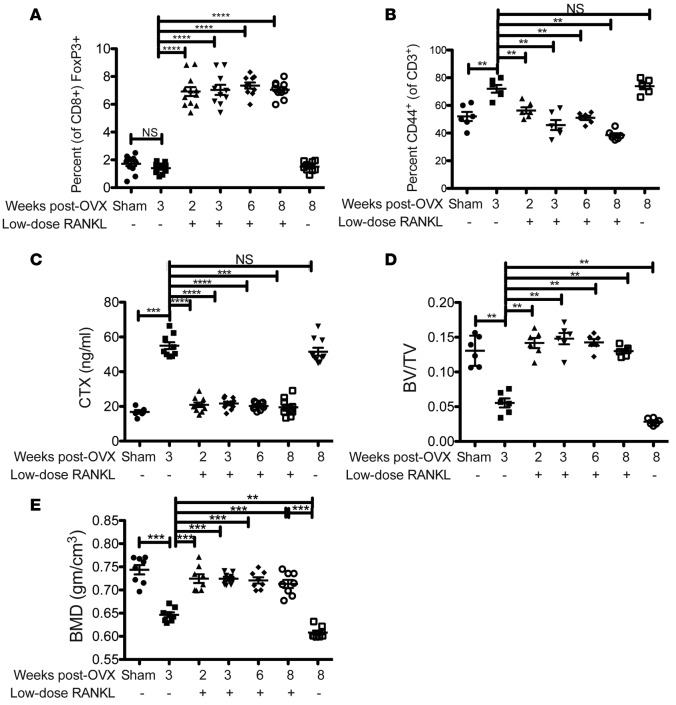
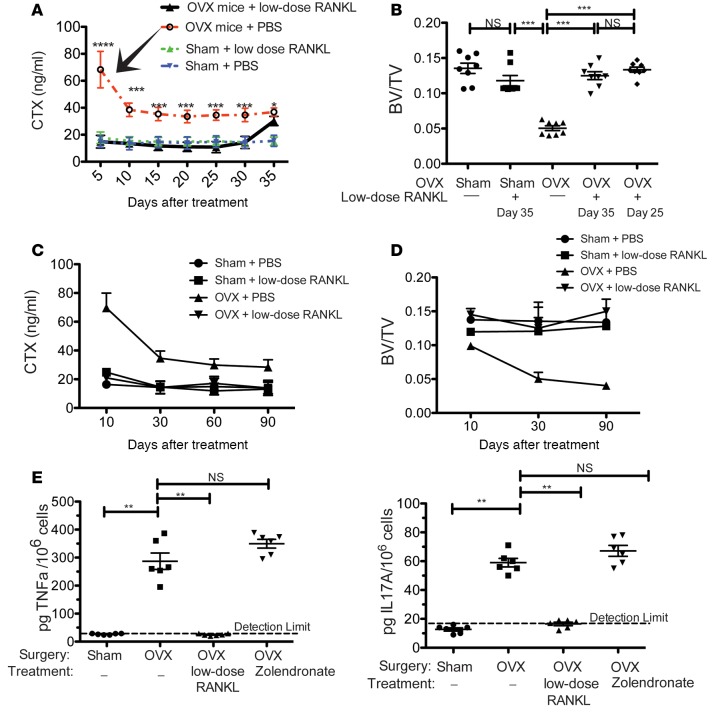
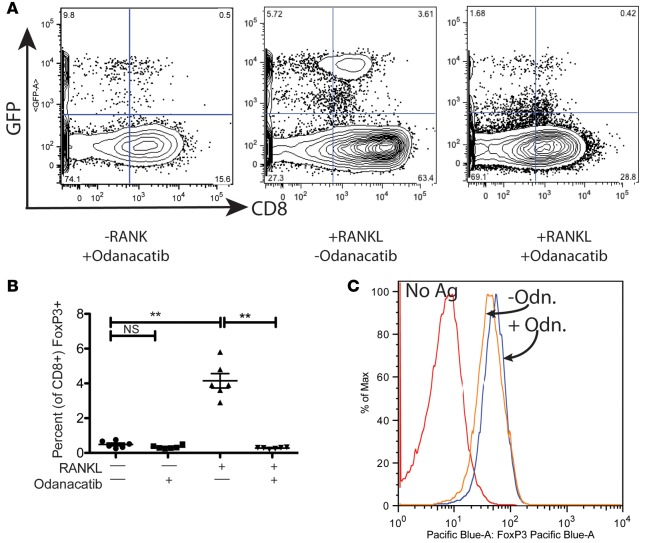
A number of studies in model animal systems and in the clinic have established that RANKL promotes bone resorption. Paradoxically, we found that pulsing ovariectomized mice with low-dose RANKL suppressed bone resorption, decreased the levels of proinflammatory effector T cells and led to increased bone mass. This effect of RANKL is mediated through the induction of FoxP3+CD25+ regulatory CD8+ T cells (TcREG) by osteoclasts. Here, we show that pulses of low-dose RANKL are needed to induce TcREG, as continuous infusion of identical doses of RANKL by pump did not induce TcREG. We also show that low-dose RANKL can induce TcREG at 2, 3, 6, and 10 weeks after ovariectomy. Our results show that low-dose RANKL treatment in ovariectomized mice is optimal at once-per-month doses to maintain the bone mass. Finally, we found that treatment of ovariectomized mice with the Cathepsin K inhibitor odanacatib also blocked TcREG induction by low-dose RANKL. We interpret this result to indicate that antigens presented to CD8+ T cells by osteoclasts are derived from the bone protein matrix because Cathepsin K degrades collagen in the bone. Taken together, our studies provide a basis for using low-dose RANKL as a potential therapeutic for postmenopausal osteoporosis.
Conflict of interest statement
ZSB and RA are listed as inventors on two patents on the use of TcREG (9144599) and the use of pulsed low-dose RANKL (pending) as therapy.
Figures
Similar articles
-
A Bone Anabolic Effect of RANKL in a Murine Model of Osteoporosis Mediated Through FoxP3+ CD8 T Cells.J Bone Miner Res. 2015 Aug;30(8):1508-22. doi: 10.1002/jbmr.2472. Epub 2015 May 21. J Bone Miner Res. 2015. PMID: 25656537 Free PMC article.
-
WSS25, a sulfated polysaccharide, inhibits RANKL-induced mouse osteoclast formation by blocking SMAD/ID1 signaling.Acta Pharmacol Sin. 2015 Sep;36(9):1053-64. doi: 10.1038/aps.2015.65. Epub 2015 Aug 24. Acta Pharmacol Sin. 2015. PMID: 26299951 Free PMC article.
-
Odanacatib, a cathepsin-K inhibitor for osteoporosis: a two-year study in postmenopausal women with low bone density.J Bone Miner Res. 2010 May;25(5):937-47. doi: 10.1359/jbmr.091035. J Bone Miner Res. 2010. PMID: 19874198 Clinical Trial.
-
Odanacatib, a cathepsin K inhibitor for the treatment of osteoporosis and other skeletal disorders associated with excessive bone remodeling.IDrugs. 2009 Dec;12(12):799-809. IDrugs. 2009. PMID: 19943223 Review.
-
Role of RANK ligand and denosumab, a targeted RANK ligand inhibitor, in bone health and osteoporosis: a review of preclinical and clinical data.Clin Ther. 2012 Mar;34(3):521-36. doi: 10.1016/j.clinthera.2012.02.002. Clin Ther. 2012. PMID: 22440513 Review.
Cited by
-
Soluble Factors on Stage to Direct Mesenchymal Stem Cells Fate.Front Bioeng Biotechnol. 2017 May 17;5:32. doi: 10.3389/fbioe.2017.00032. eCollection 2017. Front Bioeng Biotechnol. 2017. PMID: 28567372 Free PMC article. Review.
-
T-Cell Mediated Inflammation in Postmenopausal Osteoporosis.Front Immunol. 2021 Jun 30;12:687551. doi: 10.3389/fimmu.2021.687551. eCollection 2021. Front Immunol. 2021. PMID: 34276675 Free PMC article. Review.
-
Iguratimod prevents ovariectomy‑induced bone loss and suppresses osteoclastogenesis via inhibition of peroxisome proliferator‑activated receptor‑γ.Mol Med Rep. 2017 Dec;16(6):8200-8208. doi: 10.3892/mmr.2017.7648. Epub 2017 Sep 28. Mol Med Rep. 2017. PMID: 28983607 Free PMC article.
-
Immunoporosis: A New Role for Invariant Natural Killer T (NKT) Cells Through Overexpression of Nuclear Factor-κB Ligand (RANKL).Med Sci Monit. 2019 Mar 23;25:2151-2158. doi: 10.12659/MSM.912119. Med Sci Monit. 2019. PMID: 30903656 Free PMC article.
-
The Cell Surface Markers Expression in Postmenopausal Women and Relation to Obesity and Bone Status.Int J Environ Res Public Health. 2017 Jul 11;14(7):751. doi: 10.3390/ijerph14070751. Int J Environ Res Public Health. 2017. PMID: 28696349 Free PMC article.
References
-
- Dore RK. The RANKL pathway and denosumab. Rheum Dis Clin North Am. 2011;37(3):433–52. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
