

Intranasal sedatives in pediatric dentistry
- PMID: 27570849
- PMCID: PMC5039613
- DOI: 10.15537/smj.2016.9.15003
Intranasal sedatives in pediatric dentistry
Abstract
Objectives: To identify the intranasal (IN) sedatives used to achieve conscious sedation during dental procedures amongst children.
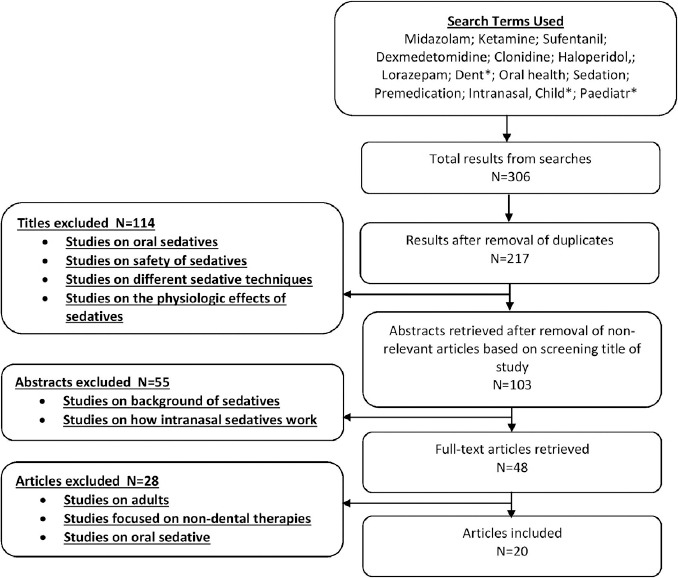
Methods: A literature review was conducted by identifying relevant studies through searches on Medline. Search included IN of midazolam, ketamine, sufentanil, dexmedetomidine, clonidine, haloperidol, and loranzepam. Studies included were conducted amongst individuals below 18 years, published in English, and were not restricted by year. Exclusion criteria were articles that did not focus on pediatric dentistry.
Results: Twenty studies were included. The most commonly used sedatives were midazolam, followed by ketamine and sufentanil. Onset of action for IN midazolam was 5-15 minutes (min), however, IN ketamine was faster (mean 5.74 min), while both IN sufentanil (mean 20 min) and IN dexmedetomidine (mean 25 min) were slow in comparison. Midazolam was effective for modifying behavior in mild to moderately anxious children, however, for more invasive or prolonged procedures, stronger sedatives, such as IN ketamine, IN sufentanil were recommended. In addition, ketamine fared better in overall success rate (89%) when compared with IN midazolam (69%). Intranasal dexmedetomidine was only used as pre-medication amongst children. While its' onset of action is longer when compared with IN midazolam, it produced deeper sedation at the time of separation from the parent and at the time of anesthesia induction.
Conclusion: Intranasal midazolam, ketamine, and sufentanil are effective and safe for conscious sedation, while intranasal midazolam, dexmedetomidine, and sufentanil have proven to be effective premedications.
Figures
Similar articles
-
Intranasal sufentanil/midazolam versus ketamine/midazolam for analgesia/sedation in the pediatric population prior to undergoing multiple dental extractions under general anesthesia: a prospective, double-blind, randomized comparison.Anesth Prog. 2004;51(4):114-21. Anesth Prog. 2004. PMID: 15675259 Free PMC article. Clinical Trial.
-
Intranasal dexmedetomidine and intranasal ketamine association allows shorter induction time for pediatric sedation compared to intranasal dexmedetomidine and oral midazolam.Ital J Pediatr. 2022 Jan 10;48(1):5. doi: 10.1186/s13052-021-01196-0. Ital J Pediatr. 2022. PMID: 35012598 Free PMC article.
-
A comparative evaluation of intranasal dexmedetomidine, midazolam and ketamine for their sedative and analgesic properties: a triple blind randomized study.J Clin Pediatr Dent. 2014 Spring;38(3):255-61. doi: 10.17796/jcpd.38.3.l828585807482966. J Clin Pediatr Dent. 2014. PMID: 25095322 Clinical Trial.
-
Comparison of different sedatives in children before general anaesthesia for selective surgery: A network meta-analysis.J Clin Pharm Ther. 2022 Oct;47(10):1495-1505. doi: 10.1111/jcpt.13763. Epub 2022 Aug 27. J Clin Pharm Ther. 2022. PMID: 36029118 Review.
-
Intranasal drug administration for procedural sedation in children admitted to pediatric Emergency Room.Eur Rev Med Pharmacol Sci. 2018 Jan;22(1):217-222. doi: 10.26355/eurrev_201801_14120. Eur Rev Med Pharmacol Sci. 2018. PMID: 29364490 Review.
Cited by
-
Remimazolam as a Novel Anesthetic in Pediatric Procedural Sedation and Anesthesia: A Narrative Review.Cureus. 2025 Jun 19;17(6):e86354. doi: 10.7759/cureus.86354. eCollection 2025 Jun. Cureus. 2025. PMID: 40688881 Free PMC article. Review.
-
Evaluation of Intranasal Midazolam for Pediatric Sedation during the Suturing of Traumatic Lacerations: A Systematic Review.Children (Basel). 2022 Apr 29;9(5):644. doi: 10.3390/children9050644. Children (Basel). 2022. PMID: 35626821 Free PMC article. Review.
-
Comparative Analysis of Intravenous Midazolam with Nasal Spray for Conscious Sedation in Minor Oral and Maxillofacial Surgeries.J Pharm Bioallied Sci. 2019 Feb;11(Suppl 1):S42-S50. doi: 10.4103/jpbs.JPBS_199_18. J Pharm Bioallied Sci. 2019. PMID: 30923430 Free PMC article.
-
Comparison of two Intranasal Sedatives, Midazolam versus Dexmedetomidine, in Children with High Dental Fear: a Randomized Clinical Trial.J Dent (Shiraz). 2022 Jun;23(2):129-136. doi: 10.30476/DENTJODS.2021.89323.1406. J Dent (Shiraz). 2022. PMID: 35783491 Free PMC article.
-
The Sedative Effects of Inhaled Nebulized Dexmedetomidine on Children: A Systematic Review and Meta-Analysis.Front Pediatr. 2022 May 20;10:865107. doi: 10.3389/fped.2022.865107. eCollection 2022. Front Pediatr. 2022. PMID: 35669400 Free PMC article.
References
-
- Chhabra N, Chhabra A, Walia G. Prevalence of dental anxiety and fear among five to ten year old children: a behaviour based cross sectional study. Minerva Stomatol. 2012;61:83–89. - PubMed
-
- Willson S. Pharmacological management of the pediatric dental patient. Pediatr Dent. 2004;26:131–136. - PubMed
-
- Lee-Kim SJ, Fadavi S, Punwani I, Koerber A. Nasal versus oral midazolam sedation for pediatric dental patients. J Dent Child (Chic) 2004;71:126–130. - PubMed
-
- Heard C, Smith J, Creighton P, Joshi P, Feldman D, Lerman J. A comparison of four sedation techniques for pediatric dental surgery. Paediatr Anaesth. 2010;20:924–930. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources