

Ten-Year Outcomes After Coronary Artery Bypass Grafting According to Age in Patients With Heart Failure and Left Ventricular Systolic Dysfunction: An Analysis of the Extended Follow-Up of the STICH Trial (Surgical Treatment for Ischemic Heart Failure)
- PMID: 27573034
- PMCID: PMC5089908
- DOI: 10.1161/CIRCULATIONAHA.116.024800
Ten-Year Outcomes After Coronary Artery Bypass Grafting According to Age in Patients With Heart Failure and Left Ventricular Systolic Dysfunction: An Analysis of the Extended Follow-Up of the STICH Trial (Surgical Treatment for Ischemic Heart Failure)
Abstract
Background: Advancing age is associated with a greater prevalence of coronary artery disease in heart failure with reduced ejection fraction and with a higher risk of complications after coronary artery bypass grafting (CABG). Whether the efficacy of CABG compared with medical therapy (MED) in patients with heart failure caused by ischemic cardiomyopathy is the same in patients of different ages is unknown.
Methods: A total of 1212 patients (median follow-up, 9.8 years) with ejection fraction ≤35% and coronary disease amenable to CABG were randomized to CABG or MED in the STICH trial (Surgical Treatment for Ischemic Heart Failure).
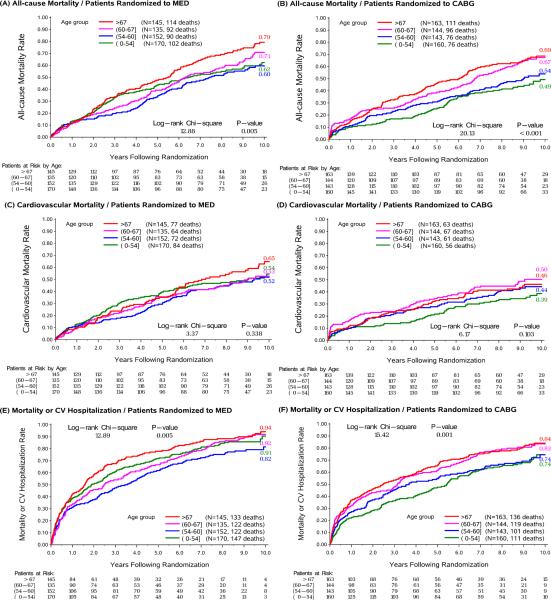
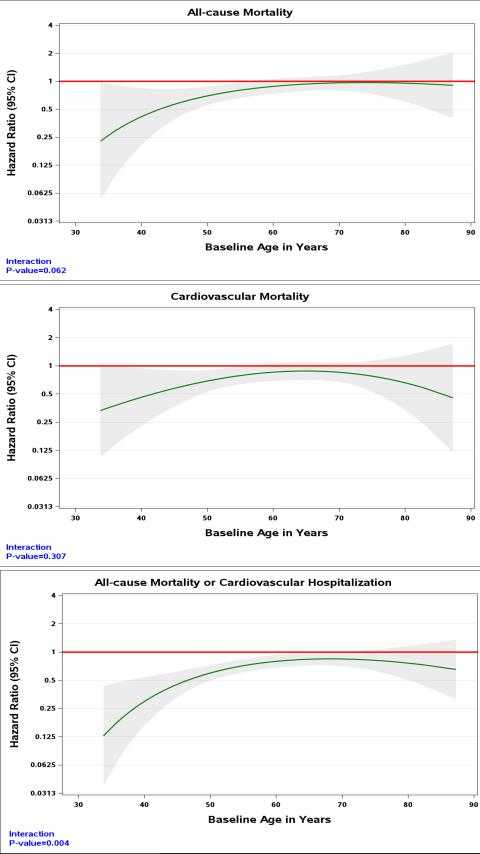
Results: Mean age at trial entry was 60 years; 12% were women; 36% were nonwhite; and the baseline ejection fraction was 28%. For the present analyses, patients were categorized by age quartiles: quartile 1, ≤54 years; quartile, 2 >54 and ≤60 years; quartile 3, >60 and ≤67 years; and quartile 4, >67 years. Older versus younger patients had more comorbidities. All-cause mortality was higher in older compared with younger patients assigned to MED (79% versus 60% for quartiles 4 and 1, respectively; log-rank P=0.005) and CABG (68% versus 48% for quartiles 4 and 1, respectively; log-rank P<0.001). In contrast, cardiovascular mortality was not statistically significantly different across the spectrum of age in the MED group (53% versus 49% for quartiles 4 and 1, respectively; log-rank P=0.388) or CABG group (39% versus 35% for quartiles 4 and 1, respectively; log-rank P=0.103). Cardiovascular deaths accounted for a greater proportion of deaths in the youngest versus oldest quartile (79% versus 62%). The effect of CABG versus MED on all-cause mortality tended to diminish with increasing age (Pinteraction=0.062), whereas the benefit of CABG on cardiovascular mortality was consistent over all ages (Pinteraction=0.307). There was a greater reduction in all-cause mortality or cardiovascular hospitalization with CABG versus MED in younger compared with older patients (Pinteraction=0.004). In the CABG group, cardiopulmonary bypass time or days in intensive care did not differ for older versus younger patients.
Conclusions: CABG added to MED has a more substantial benefit on all-cause mortality and the combination of all-cause mortality and cardiovascular hospitalization in younger compared with older patients. CABG added to MED has a consistent beneficial effect on cardiovascular mortality regardless of age.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT00023595.
Keywords: aging; coronary artery bypass; coronary artery disease; heart failure.
© 2016 American Heart Association, Inc.
Figures
Comment in
-
An Age-Old Question: What Is Too Old for Coronary Artery Bypass Grafting in Heart Failure?Circulation. 2016 Nov 1;134(18):1325-1327. doi: 10.1161/CIRCULATIONAHA.116.024878. Circulation. 2016. PMID: 27799256 No abstract available.
Similar articles
-
Sex Difference in Patients With Ischemic Heart Failure Undergoing Surgical Revascularization: Results From the STICH Trial (Surgical Treatment for Ischemic Heart Failure).Circulation. 2018 Feb 20;137(8):771-780. doi: 10.1161/CIRCULATIONAHA.117.030526. Circulation. 2018. PMID: 29459462 Free PMC article. Clinical Trial.
-
Influence of Baseline Characteristics, Operative Conduct, and Postoperative Course on 30-Day Outcomes of Coronary Artery Bypass Grafting Among Patients With Left Ventricular Dysfunction: Results From the Surgical Treatment for Ischemic Heart Failure (STICH) Trial.Circulation. 2015 Aug 25;132(8):720-30. doi: 10.1161/CIRCULATIONAHA.114.014932. Circulation. 2015. PMID: 26304663 Free PMC article. Clinical Trial.
-
Coronary-Artery Bypass Surgery in Patients with Ischemic Cardiomyopathy.N Engl J Med. 2016 Apr 21;374(16):1511-20. doi: 10.1056/NEJMoa1602001. Epub 2016 Apr 3. N Engl J Med. 2016. PMID: 27040723 Free PMC article. Clinical Trial.
-
Do patients with heart failure benefit from coronary artery bypass grafting?Curr Opin Cardiol. 2012 Nov;27(6):629-33. doi: 10.1097/HCO.0b013e328358b08d. Curr Opin Cardiol. 2012. PMID: 23032716 Review.
-
A review of the Surgical Treatment for Ischemic Heart Failure trial.Asian Cardiovasc Thorac Ann. 2020 Nov;28(9):633-637. doi: 10.1177/0218492320957162. Epub 2020 Sep 1. Asian Cardiovasc Thorac Ann. 2020. PMID: 32870026 Review.
Cited by
-
Within trial comparison of survival time projections from short-term follow-up with long-term follow-up findings.ESC Heart Fail. 2022 Oct;9(5):3655-3658. doi: 10.1002/ehf2.13731. Epub 2022 Jul 7. ESC Heart Fail. 2022. PMID: 35799450 Free PMC article.
-
The Role of Positron Emission Tomography in Advancing the Understanding of the Pathogenesis of Heart and Vascular Diseases.Diagnostics (Basel). 2023 May 18;13(10):1791. doi: 10.3390/diagnostics13101791. Diagnostics (Basel). 2023. PMID: 37238275 Free PMC article. Review.
-
Percutaneous Coronary Intervention for Heart Failure: Worth the Cost?Circ Cardiovasc Qual Outcomes. 2024 Jan;17(1):e010572. doi: 10.1161/CIRCOUTCOMES.123.010572. Epub 2023 Nov 6. Circ Cardiovasc Qual Outcomes. 2024. PMID: 37929590 Free PMC article. No abstract available.
-
Best evidence for coronary revascularization - multisociety endorsement of the 2024 ESC guidelines.Indian J Thorac Cardiovasc Surg. 2025 Jul;41(7):826-829. doi: 10.1007/s12055-025-01971-2. Epub 2025 May 8. Indian J Thorac Cardiovasc Surg. 2025. PMID: 40535227 No abstract available.
-
CABG in patients with left ventricular dysfunction: indications, techniques and outcomes.Indian J Thorac Cardiovasc Surg. 2018 Dec;34(Suppl 3):279-286. doi: 10.1007/s12055-018-0738-8. Epub 2018 Oct 17. Indian J Thorac Cardiovasc Surg. 2018. PMID: 33060950 Free PMC article. Review.
References
-
- Wong CM, Hawkins NM, Petrie MC, Jhund PS, Gardner RS, Ariti CA, Poppe KK, Earle N, Whalley GA, Squire IB, Doughty RN, McMurray JJV. Heart failure in younger patients: the Meta-analysis Global Group in Chronic Heart Failure (MAGGIC). Eur Heart J. 2014;35:2714–2721. - PubMed
-
- Shafazand M, Schaufelberger M, Lappas G, Swedberg K, Rosengren A. Survival trends in men and women with heart failure of ischaemic and non-ischaemic origin: data for the period 1987-2003 from the Swedish Hospital Discharge Registry. Eur Heart J. 2009;30:671–8. - PubMed
-
- Velazquez EJ, Lee KL, Deja MA, Jain A, Sopko G, Marchenko A, Ali IS, Pohost G, Gradinac S, Abraham WT, Yii M, Prabhakaran D, Szwed H, Ferrazzi P, Petrie MC, O'Connor CM, Panchavinnin P, She L, Bonow RO, Rankin GR, Jones RH, Rouleau J-L. Coronary-Artery Bypass Surgery in Patients with Left Ventricular Dysfunction. N Engl J Med. 2011;364:1607–1616. - PMC - PubMed
-
- Velazquez EJ, Lee KL, Jones RH, Al-Khalidi HR, Hill JA, Panza JA, Michler RE, Bonow RO, Doenst T, Petrie MC, Oh JK, She L, Moore VL, Desvigne-Nickens P, Sopko G, Rouleau JL. STICHES Investigators. Coronary-Artery Bypass Surgery in Patients with Ischemic Cardiomyopathy. N Engl J Med. 2016;374:1511–20. - PMC - PubMed
-
- Chung PJ, Carter TI, Burack JH, Tam S, Alfonso A, Sugiyama G. Predicting the risk of death following coronary artery bypass graft made simple: a retrospective study using the American College of Surgeons National Surgical Quality Improvement Program database. J Cardiothorac Surg. 2015;10:62. - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
