

Extramedullary Disease in Adult Acute Myeloid Leukemia Is Common but Lacks Independent Significance: Analysis of Patients in ECOG-ACRIN Cancer Research Group Trials, 1980-2008
- PMID: 27573652
- PMCID: PMC5074349
- DOI: 10.1200/JCO.2016.67.5892
Extramedullary Disease in Adult Acute Myeloid Leukemia Is Common but Lacks Independent Significance: Analysis of Patients in ECOG-ACRIN Cancer Research Group Trials, 1980-2008
Erratum in
-
Errata.J Clin Oncol. 2017 Jan 10;35(2):263. doi: 10.1200/JCO.2016.71.6407. J Clin Oncol. 2017. PMID: 31305609 Free PMC article.
Abstract
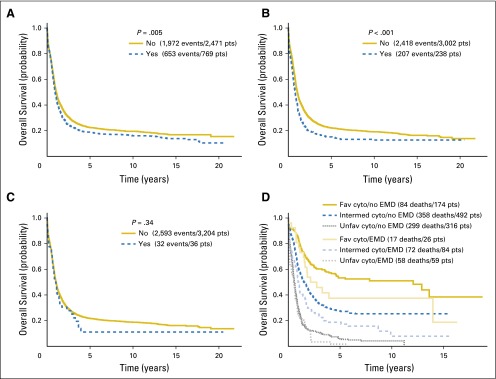
Purpose Extramedullary disease (EMD) at diagnosis in patients with acute myeloid leukemia (AML) has been recognized for decades. Reported herein are results from a large study of patients with AML who were treated in consecutive ECOG-ACRIN Cancer Research Group frontline clinical trials in an attempt to define the incidence and clinical implications of EMD. Methods Patients with newly diagnosed AML, age 15 years and older, who were treated in 11 clinical trials, were studied to identify EMD, as defined by physical examination, laboratory findings, and imaging results. Results Of the 3,522 patients enrolled, 282 were excluded, including patients with acute promyelocytic leukemia, incorrect diagnosis, or no adequate assessment of EMD at baseline. The overall incidence of EMD was 23.7%. The sites involved were: lymph nodes (11.5%), spleen (7.3%), liver (5.3%), skin (4.5%), gingiva (4.4%), and CNS (1.1%). Most patients (65.3%) had only one site of EMD, 20.9% had two sites, 9.5% had three sites, and 3.4% had four sites. The median overall survival was 1.035 years. In univariable analysis, the presence of any EMD ( P = .005), skin involvement ( P = .002), spleen ( P < .001), and liver ( P < .001), but not CNS ( P = .34), nodal involvement ( P = .94), and gingival hypertrophy ( P = .24), was associated with a shorter overall survival. In contrast, in multivariable analysis, adjusted for known prognostic factors such as cytogenetic risk and WBC count, neither the presence of EMD nor the number of specific sites of EMD were independently prognostic. Conclusion This large study demonstrates that EMD at any site is common but is not an independent prognostic factor. Treatment decisions for patients with EMD should be made on the basis of recognized AML prognostic factors, irrespective of the presence of EMD.
Conflict of interest statement
Authors’ disclosures of potential conflicts of interest are found in the article online at www.jco.org. Author contributions are found at the end of this article.
Figures
References
-
- Muss HB, Moloney WC. Chloroma and other myeloblastic tumors. Blood. 1973;42:721–728. - PubMed
-
- Chang H, Brandwein J, Yi QL, et al. Extramedullary infiltrates of AML are associated with CD56 expression, 11q23 abnormalities and inferior clinical outcome. Leuk Res. 2004;28:1007–1011. - PubMed
-
- Tallman MS, Kim HT, Paietta E, et al. Acute monocytic leukemia (French-American-British classification M5) does not have a worse prognosis than other subtypes of acute myeloid leukemia: A report from the Eastern Cooperative Oncology Group. J Clin Oncol. 2004;22:1276–1286. - PubMed
-
- Tallman MS, Hakimian D, Shaw JM, et al. Granulocytic sarcoma is associated with the 8;21 translocation in acute myeloid leukemia. J Clin Oncol. 1993;11:690–697. - PubMed
-
- Byrd JC, Weiss RB, Arthur DC, et al. Extramedullary leukemia adversely affects hematologic complete remission rate and overall survival in patients with t(8;21)(q22;q22): Results from Cancer and Leukemia Group B 8461. J Clin Oncol. 1997;15:466–475. - PubMed
Publication types
MeSH terms
Grants and funding
- U10 CA013650/CA/NCI NIH HHS/United States
- U10 CA014958/CA/NCI NIH HHS/United States
- U24 CA196172/CA/NCI NIH HHS/United States
- U10 CA049883/CA/NCI NIH HHS/United States
- U10 CA017145/CA/NCI NIH HHS/United States
- U10 CA180795/CA/NCI NIH HHS/United States
- U10 CA066636/CA/NCI NIH HHS/United States
- U10 CA180790/CA/NCI NIH HHS/United States
- U10 CA073590/CA/NCI NIH HHS/United States
- U10 CA180794/CA/NCI NIH HHS/United States
- U10 CA021115/CA/NCI NIH HHS/United States
- UG1 CA189859/CA/NCI NIH HHS/United States
- P30 CA008748/CA/NCI NIH HHS/United States
- U10 CA180791/CA/NCI NIH HHS/United States
- U10 CA023318/CA/NCI NIH HHS/United States
- U10 CA014548/CA/NCI NIH HHS/United States
- U10 CA180820/CA/NCI NIH HHS/United States
- U10 CA015488/CA/NCI NIH HHS/United States
- U10 CA180853/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
